
Search
- Page Path
- HOME > Search
Original Articles
- Clinical outcomes of combined phacoemulsification and epiretinal membrane peeling using three advanced intraocular lens platforms
- Chan Hong Min, Jaehyuck Jo, Ho Seok Chung, Dong Yoon Kim, Jin Hyoung Park
- Insights Cataract Refract Surg 2026;11(2):47-55. Published online May 21, 2026
- DOI: https://doi.org/10.63375/icrs.26.001
-
 Abstract
Abstract
 PDF
PDF ePub
ePub - Purpose
This retrospective study evaluated the clinical outcomes of combined phacoemulsification, implantation of 1 of 3 types of advanced intraocular lenses (IOLs) with multifocality, and pars plana vitrectomy with epiretinal membrane (ERM) peeling in patients with cataract and ERM. Outcomes were compared with those in age-matched controls who underwent phacoemulsification with the same IOL alone.
Methods
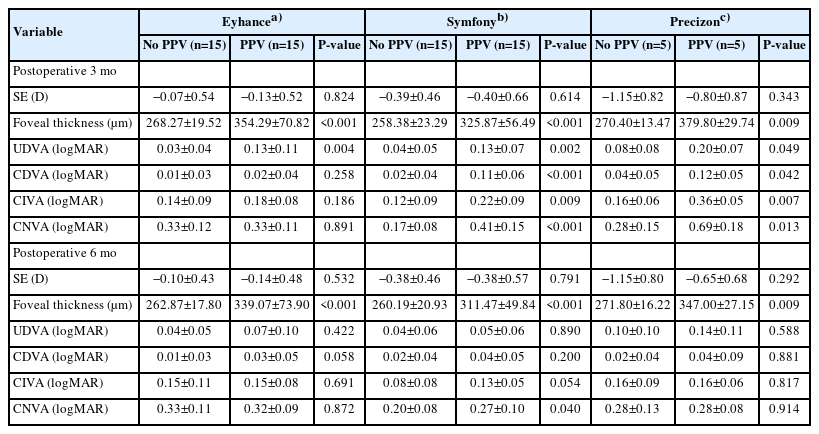
A total of 70 eyes were included: 35 eyes underwent combined surgery, and 35 served as controls. In each group, 15 eyes received an advanced monofocal IOL (Tecnis Eyhance ICB00), 15 received a hybrid diffractive extended-depth-of-focus (EDoF) IOL (Tecnis Symfony ZXR00), and five received a hybrid refractive EDoF IOL (Precizon Presbyopic NVA).
Results
All groups showed significant visual improvement by 6 months postoperatively. Eyes that received hybrid diffractive EDoF IOLs and underwent combined surgery showed significantly worse mean corrected distance visual acuity, uncorrected distance visual acuity, corrected intermediate visual acuity, and corrected near visual acuity at 3 months than control eyes, but these outcomes improved to levels comparable to those of control eyes by 6 months. Eyes that received hybrid refractive EDoF IOLs showed similar early delays; however, interpretation was limited by the small sample size.
Conclusion
Overall, combined surgery was safe and effective, although early visual recovery may be delayed in eyes receiving EDoF IOLs. These findings suggest that advanced monofocal and EDoF IOLs may be considered in selected patients with ERM; however, the results should be interpreted cautiously because of the retrospective design and limited sample size.
- 334 View
- 6 Download

- Impact of anterior chamber depth to axial length ratio on conventional intraocular lens power calculation formulas performance in axial myopia
- Youngsub Eom, Jinhwan Park, Youngbin Song, Dong Hyun Kim, Jong Suk Song
- Insights Cataract Refract Surg 2026;11(1):15-22. Published online February 26, 2026
- DOI: https://doi.org/10.63375/icrs.25.017
-
Abstract
PDFePub
- Purpose
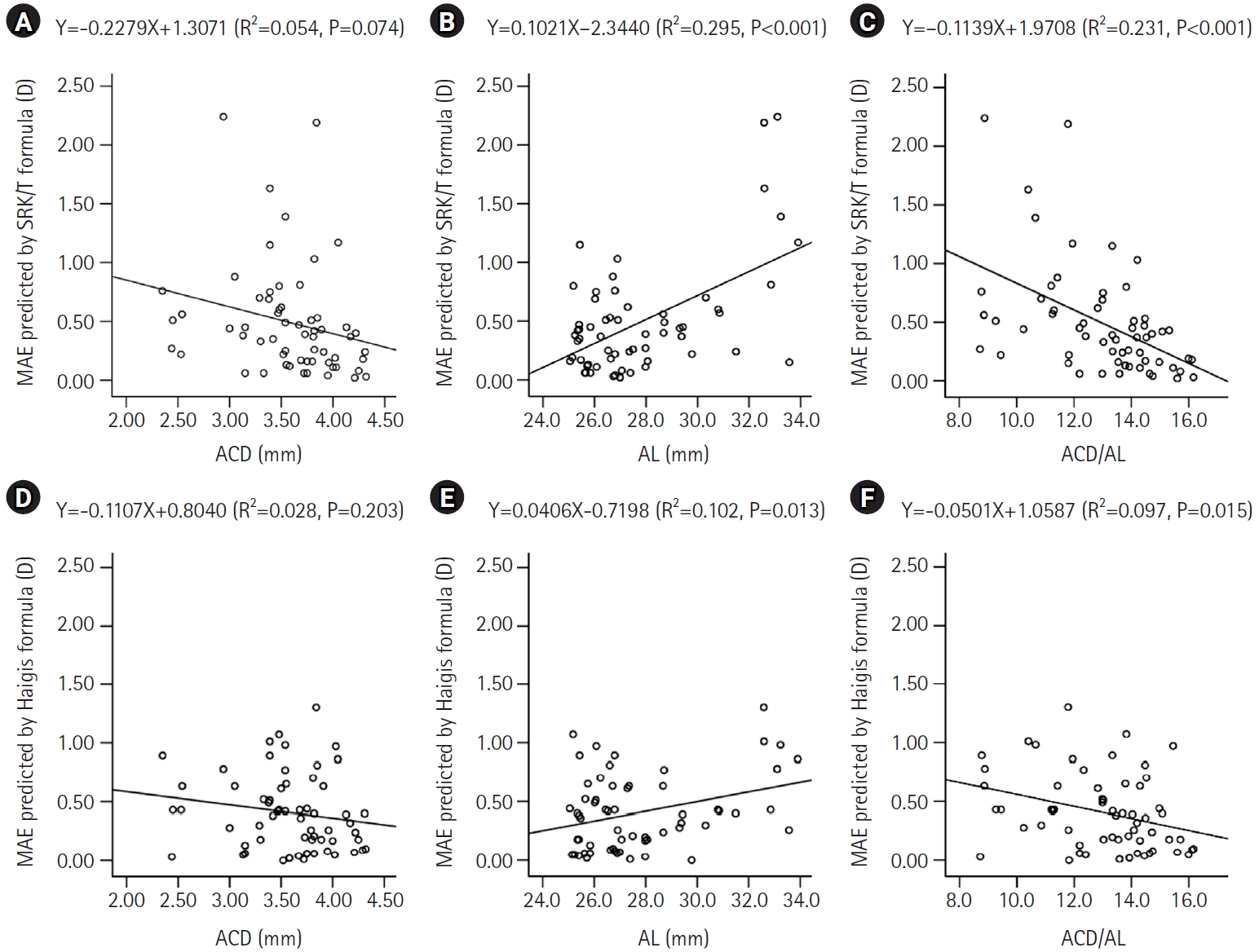
To evaluate the effects of the ratio of anterior chamber depth to axial length (ACD/AL), as well as axial length (AL) itself, on the accuracy of conventional intraocular lens (IOL) power calculation formulas in eyes with axial myopia.
Methods
This retrospective cross-sectional study included 60 eyes from 44 patients with an AL greater than 25.0 mm who underwent uncomplicated phacoemulsification with IOL implantation. Eyes were categorized into high and low AL groups using an AL threshold of 27.0 mm, and into high and low ACD/AL groups based on the median ACD/AL value of 13.4. The median absolute errors (MedAEs) predicted by the Sanders-Retzlaff-Kraff theoretical (SRK/T) and Haigis formulas were compared according to AL and ACD/AL groupings.
Results
In the low ACD/AL group and in the high AL group, the MedAEs predicted by the Haigis formula were lower than those predicted by the SRK/T formula (P=0.002 and P=0.012, respectively). The MedAEs predicted by both the SRK/T and Haigis formulas were significantly lower in the high ACD/AL group than in the low ACD/AL group (P<0.001 and P=0.010, respectively). In contrast, no significant difference was observed between the low and high AL groups in the MedAEs predicted by the Haigis formula. When the ACD/AL ratio was less than 13.4, postoperative refractive outcomes were more hyperopic with both formulas.
Conclusion
In eyes with a long AL and a relatively shallow ACD, the Haigis formula demonstrated superior accuracy among conventional IOL power calculation formulas. Under these anatomical conditions, targeting slightly more myopic postoperative refractions may therefore be advisable.
- 595 View
- 7 Download
Review Article
- Presbyopia-correcting intraocular lens options in myopic eyes undergoing cataract surgery
- Sang Beom Han
- Insights Cataract Refract Surg 2026;11(1):1-8. Published online February 26, 2026
- DOI: https://doi.org/10.63375/icrs.25.016
-
Abstract
PDFePub
- With ongoing advancements in surgical techniques and intraocular lens (IOLs) technologies, cataract surgery is increasingly recognized as a form of refractive procedure aimed at enhancing overall visual performance rather than being viewed solely as lens extraction. In parallel with this shift, a growing number of aging individuals with myopia are actively seeking spectacle independence following cataract surgery. The selection of IOLs for presbyopia correction in patients with myopia presents distinct clinical and refractive challenges, necessitating careful preoperative evaluation and individualized surgical planning. In this review, the author summarizes current evidence regarding the use of various IOLs, including monofocal, enhanced monofocal, extended depth-of-focus, and multifocal IOLs, for presbyopia correction in myopic patients and discusses key considerations involved in selecting the most appropriate IOL for this specific population.
- 563 View
- 8 Download
Original Articles
- Results of multifocal intraocular lens implantation in patients who underwent corneal refractive surgery
- Eun Chul Kim
- Insights Cataract Refract Surg 2025;10(3):76-82. Published online October 31, 2025
- DOI: https://doi.org/10.63375/icrs.25.011
-
Abstract
PDFePub
- Purpose
The aim of this study was to evaluate the clinical results of multifocal intraocular lenses in patients who underwent corneal refractive surgery.
Methods
Thirty eyes (16 patients; Synergy: ZFR00V) were retrospectively enrolled. Uncorrected and corrected near visual acuity (UNVA, CNVA), intermediate visual acuity (UIVA, CIVA), and distant visual acuity (UDVA, CDVA), manifest refraction spherical equivalent (MRSE), and satisfaction score were assessed before and after surgery.
Results
The postoperative UDVA, UIVA, UNVA, and MRSE of the three groups exhibited improvements compared to the preoperative data (P<0.05). The error between the postoperative refraction and the intraocular lens calculation was smaller with the Barrett True K formula than with the Haigis-L formula (P<0.05). The defocus curve at 0 diopter (D) increased, from –1 to –1.5 D, and from –2.5 to –4.0 D, indicating improved vision at distant, intermediate, and near distances. Distance satisfaction (1.47±0.63), near satisfaction (1.25±0.71), and overall satisfaction (1.36±0.42) were good, but light scattering and halo satisfaction (1.97±0.85) yielded a poor result.
Conclusion
In patients with cataracts who underwent corneal refractive surgery, multifocal intraocular lens implantation resulted in excellent uncorrected visual acuity at distant, intermediate, and near distances. However, careful consideration should be given to patient selection due to the incidence of side effects such as glare and halos.
- 914 View
- 14 Download
- Efficacy of extended depth of focus, enhanced monofocal, and monofocal intraocular lenses in patients with retinal disease
- Eun Chul Kim
- Insights Cataract Refract Surg 2025;10(2):52-60. Published online June 30, 2025
- DOI: https://doi.org/10.63375/icrs.25.009
-
Abstract
PDFePub
- Purpose
The aim of this study was to compare the visual quality of extended depth of focus (EDOF), enhanced monofocal, and monofocal intraocular lenses (IOLs) in patients with retinal disease.
Methods
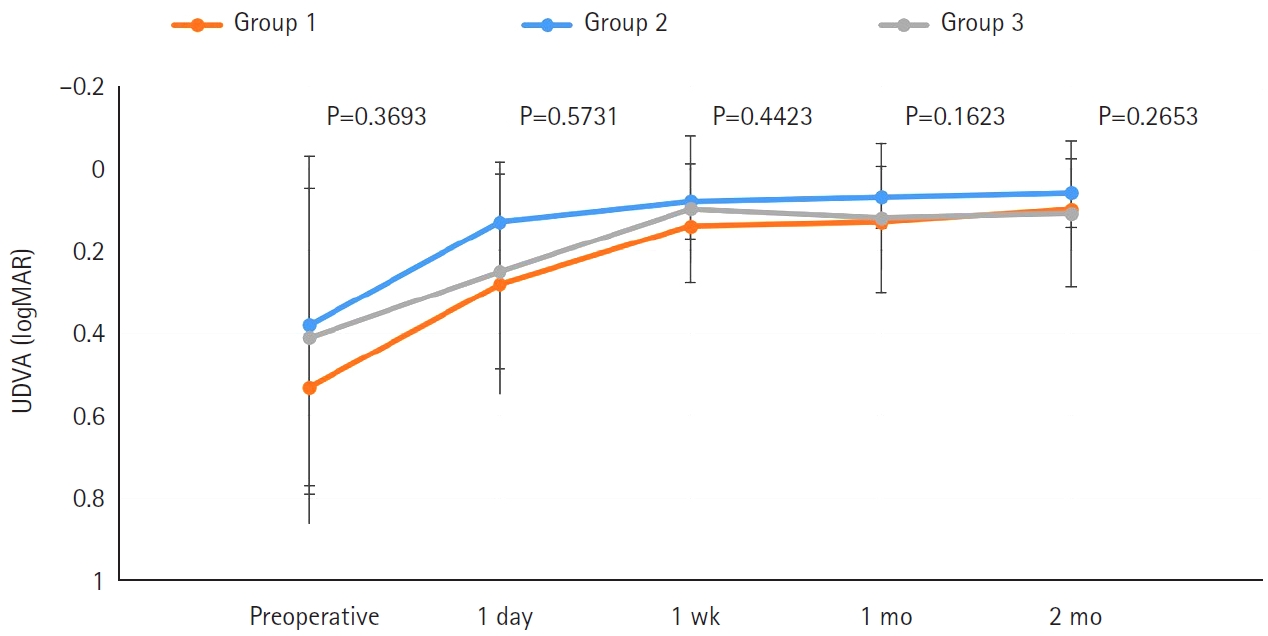
In total, 103 eyes from 93 patients (group 1: enhanced monofocal ICB00, n=36; group 2: EDOF ZXR00, n=36; group 3: monofocal ZCB00, n=31) were retrospectively enrolled. Uncorrected and corrected near visual acuity (UNVA, CNVA), intermediate visual acuity (UIVA, CIVA), and distance visual acuity (UDVA, CDVA), manifest refraction spherical equivalent (MRSE), and satisfaction scores were assessed before and after surgery.
Results
The postoperative UDVA, CDVA, and MRSE of the three groups were better than the preoperative data, respectively (P<0.05). The UIVA of group 1 (0.13±0.12 logMAR) and 2 (0.10±0.11) was significantly better than that of groups 3 (0.25±0.15) (P<0.05). The UNVA of group 2 (0.18±0.12) was significantly better than that of groups 1 (0.32±0.20) and 3 (0.45±0.26; P<0.05). The UDVA of patients with macular edema and macular holes was insignificantly lower than that of epiretinal membranes and high myopia. The overall satisfaction of group 1 (1.58±0.81) and 2 (1.46±0.75) was significantly better than that of groups 3 (1.83±0.97; P<0.05).
Conclusion
EDOF and enhanced monofocal IOLs were associated with better intermediate and near vision than monofocal IOLs in patients with retinal disease. However, monofocal IOLs are recommended in patients with macular edema and macular holes, unlike patients with epiretinal membranes and high myopia.
- 1,577 View
- 22 Download
Review Article
- Selection of an optimal intraocular lens according to the stage of epiretinal membrane
- Sang Beom Han
- Insights Cataract Refract Surg 2025;10(1):7-12. Published online February 28, 2025
- DOI: https://doi.org/10.63375/icrs.25.003
-
Abstract
PDFePub
- Epiretinal membrane (ERM), one of the most common retinal diseases, can cause various degrees of visual disturbance, reduced contrast sensitivity, and metamorphopsia. ERM is not infrequently encountered during preoperative evaluations for cataract surgery, and selecting an appropriate intraocular lens (IOL) according to the location and stage of ERM is necessary in order to improve visual outcomes and patients’ satisfaction. This review summarizes the application of various IOLs—such as multifocal, extended depth of focus, and enhanced monofocal IOLs—in eyes with ERM, and discusses the selection of an appropriate IOL.
-
Citations
Citations to this article as recorded by
- Presbyopia-correcting intraocular lens options in myopic eyes undergoing cataract surgery
Sang Beom Han
Insights in Cataract and Refractive Surgery.2026; 11(1): 1. CrossRef
- Presbyopia-correcting intraocular lens options in myopic eyes undergoing cataract surgery
- 1,816 View
- 19 Download
- 1 Crossref
 First
First Prev
Prev

