
Articles
- Page Path
- HOME > Insights Cataract Refract Surg > Volume 11(2); 2026 > Article
-
Original Article
- Clinical outcomes of combined phacoemulsification and epiretinal membrane peeling using three advanced intraocular lens platforms
-
Chan Hong Min1, Jaehyuck Jo1, Ho Seok Chung2,3, Dong Yoon Kim4, Jin Hyoung Park1,3

-
Insights in Cataract and Refractive Surgery 2026;11(2):47-55.
DOI: https://doi.org/10.63375/icrs.26.001
Published online: May 21, 2026
1MS Eye Clinic, Seoul, Korea
2Department of Ophthalmology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
3Research Institute for Biomacromolecules, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
4Top Retina Center, Cheongju, Korea
- Correspondence to: Jin Hyoung Park MS Eye Clinic, 189 Sinbanpo-ro, Seocho-gu, Seoul 06512, Korea Tel: +82-2-6949-3322E-mail: drpark99@naver.com
• Received: February 15, 2026 • Revised: April 8, 2026 • Accepted: April 8, 2026
© 2026 Korean Society of Cataract and Refractive Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 330 Views
- 6 Download
Abstract
-
Purpose
- This retrospective study evaluated the clinical outcomes of combined phacoemulsification, implantation of 1 of 3 types of advanced intraocular lenses (IOLs) with multifocality, and pars plana vitrectomy with epiretinal membrane (ERM) peeling in patients with cataract and ERM. Outcomes were compared with those in age-matched controls who underwent phacoemulsification with the same IOL alone.
-
Methods
- A total of 70 eyes were included: 35 eyes underwent combined surgery, and 35 served as controls. In each group, 15 eyes received an advanced monofocal IOL (Tecnis Eyhance ICB00), 15 received a hybrid diffractive extended-depth-of-focus (EDoF) IOL (Tecnis Symfony ZXR00), and five received a hybrid refractive EDoF IOL (Precizon Presbyopic NVA).
-
Results
- All groups showed significant visual improvement by 6 months postoperatively. Eyes that received hybrid diffractive EDoF IOLs and underwent combined surgery showed significantly worse mean corrected distance visual acuity, uncorrected distance visual acuity, corrected intermediate visual acuity, and corrected near visual acuity at 3 months than control eyes, but these outcomes improved to levels comparable to those of control eyes by 6 months. Eyes that received hybrid refractive EDoF IOLs showed similar early delays; however, interpretation was limited by the small sample size.
-
Conclusion
- Overall, combined surgery was safe and effective, although early visual recovery may be delayed in eyes receiving EDoF IOLs. These findings suggest that advanced monofocal and EDoF IOLs may be considered in selected patients with ERM; however, the results should be interpreted cautiously because of the retrospective design and limited sample size.
Introduction
Methods
Results
Discussion
Article Information
Author contributions
Conceptualization: JHP. Data curation: JHP. Formal analysis: CHM, JHP. Methodology: JHP. Project administration: JHP. Supervision: JHP. Writing – original draft: CHM, JJ, HSC, JHP. Writing – review & editing: all authors. Final approval of the manuscript: all authors.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Fig. 1.Defocus curves of the three intraocular lens types at 6 months postoperatively. (A) Eyes that underwent pars plana vitrectomy with epiretinal membrane (ERM) peeling. (B) Control eyes. D, diopter; logMAR, logarithm of the minimum angle of resolution. a)Advanced monofocal intraocular lens (IOL) group; b)Hybrid diffractive extended-depth-of-focus (EDoF) IOL group; c)Hybrid refractive EDoF IOL.
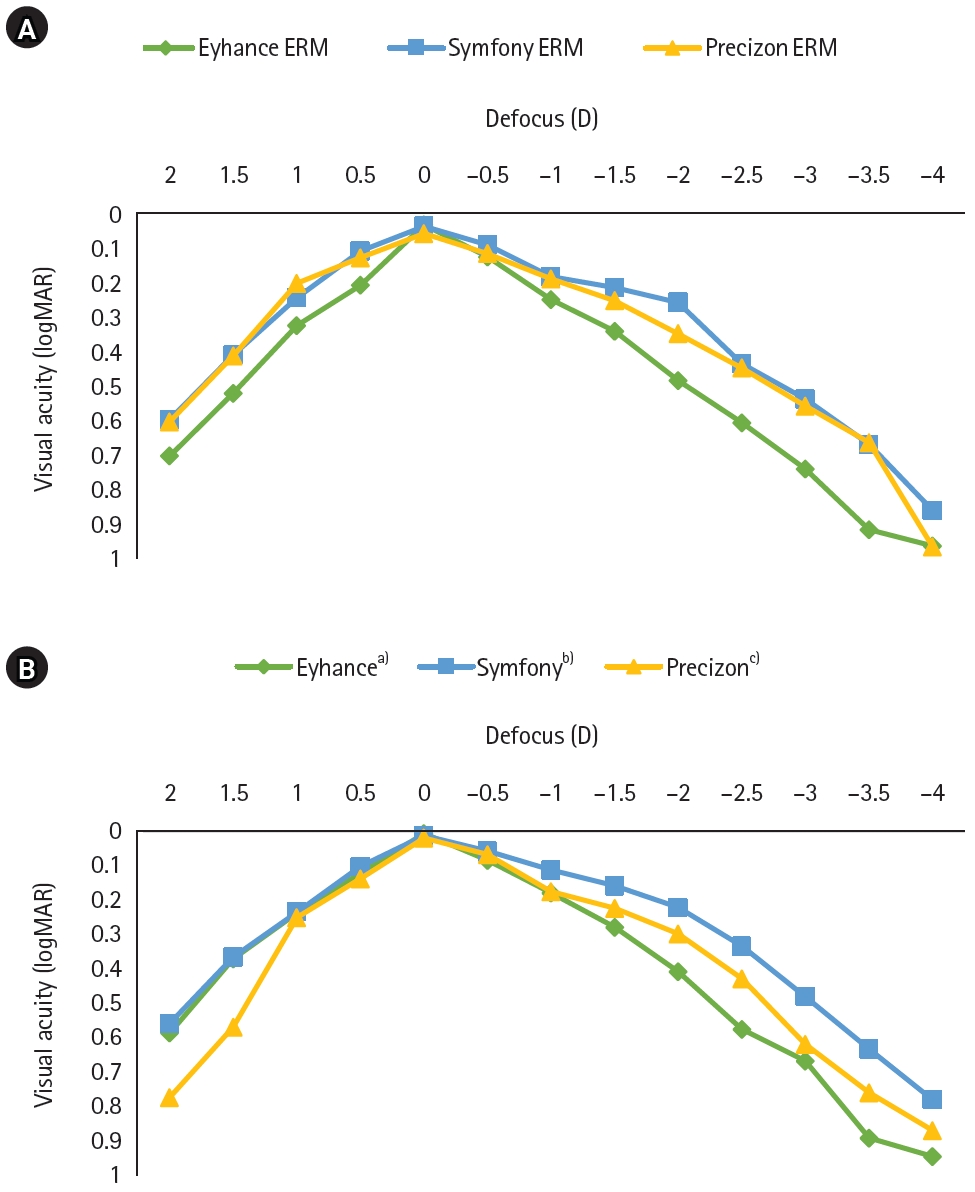
Table 1.Demographics and preoperative clinical characteristics of the study patients at baseline
| Demographic | Eyhancea) | Symfonyb) | Precizonc) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| No PPV (n=15) | PPV (n=15) | P-value | No PPV (n=15) | PPV (n=15) | P-value | No PPV (n=5) | PPV (n=5) | P-value | |
| Age (yr) | 68.07±6.18 | 67.93±11.17 | 0.847 | 62.00±6.92 | 60.40±5.60 | 0.487 | 65.00±9.27 | 67.00±5.10 | 0.684 |
| Sex, male/female | 8/7 | 7/8 | 0.726 | 5/10 | 4/11 | 0.787 | 1/4 | 2/3 | 0.545 |
| SE (D) | −0.40±1.81 | −0.18±2.28 | 0.694 | −1.52±4.42 | −1.37±4.20 | 0.781 | −0.85±1.38 | 0.75±0.85 | 0.014 |
| Foveal thickness (µm) | 263.00±18.45 | 360.50±80.82 | <0.001 | 256.31±23.41 | 333.73±61.49 | <0.001 | 273.40±17.42 | 396.00±36.55 | 0.009 |
| UDVA (logMAR) | 0.19±0.18 | 0.64±0.42 | 0.001 | 0.16±0.08 | 0.58±0.71 | <0.001 | 0.18±0.09 | 0.28±0.08 | 0.100 |
| CDVA (logMAR) | 0.09±0.11 | 0.37±0.35 | 0.001 | 0.12±0.06 | 0.16±0.05 | 0.015 | 0.18±0.09 | 0.16±0.06 | 0.911 |
| CNVA (logMAR) | 0.62±0.23 | 0.62±0.25 | 0.733 | 0.60±0.21 | 0.61±0.18 | 0.678 | 0.52±0.18 | 0.76±0.15 | 0.054 |
Values are presented as mean±standard deviation. Visual acuity is expressed as logarithm of the minimum angle of resolution (logMAR).
PPV, pars plana vitrectomy; SE, spherical equivalent; D, diopter; UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; CNVA, corrected near visual acuity.
a)Advanced monofocal intraocular lens (IOL) group;
b)Hybrid diffractive extended-depth-of-focus (EDoF) IOL group;
c)Hybrid refractive EDoF IOL.
Table 2.Postoperative visual acuity, refraction, and foveal thickness compared with controls
| Variable | Eyhancea) | Symfonyb) | Precizonc) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| No PPV (n=15) | PPV (n=15) | P-value | No PPV (n=15) | PPV (n=15) | P-value | No PPV (n=5) | PPV (n=5) | P-value | |
| Postoperative 3 mo | |||||||||
| SE (D) | −0.07±0.54 | −0.13±0.52 | 0.824 | −0.39±0.46 | −0.40±0.66 | 0.614 | −1.15±0.82 | −0.80±0.87 | 0.343 |
| Foveal thickness (µm) | 268.27±19.52 | 354.29±70.82 | <0.001 | 258.38±23.29 | 325.87±56.49 | <0.001 | 270.40±13.47 | 379.80±29.74 | 0.009 |
| UDVA (logMAR) | 0.03±0.04 | 0.13±0.11 | 0.004 | 0.04±0.05 | 0.13±0.07 | 0.002 | 0.08±0.08 | 0.20±0.07 | 0.049 |
| CDVA (logMAR) | 0.01±0.03 | 0.02±0.04 | 0.258 | 0.02±0.04 | 0.11±0.06 | <0.001 | 0.04±0.05 | 0.12±0.05 | 0.042 |
| CIVA (logMAR) | 0.14±0.09 | 0.18±0.08 | 0.186 | 0.12±0.09 | 0.22±0.09 | 0.009 | 0.16±0.06 | 0.36±0.05 | 0.007 |
| CNVA (logMAR) | 0.33±0.12 | 0.33±0.11 | 0.891 | 0.17±0.08 | 0.41±0.15 | <0.001 | 0.28±0.15 | 0.69±0.18 | 0.013 |
| Postoperative 6 mo | |||||||||
| SE (D) | −0.10±0.43 | −0.14±0.48 | 0.532 | −0.38±0.46 | −0.38±0.57 | 0.791 | −1.15±0.80 | −0.65±0.68 | 0.292 |
| Foveal thickness (µm) | 262.87±17.80 | 339.07±73.90 | <0.001 | 260.19±20.93 | 311.47±49.84 | <0.001 | 271.80±16.22 | 347.00±27.15 | 0.009 |
| UDVA (logMAR) | 0.04±0.05 | 0.07±0.10 | 0.422 | 0.04±0.06 | 0.05±0.06 | 0.890 | 0.10±0.10 | 0.14±0.11 | 0.588 |
| CDVA (logMAR) | 0.01±0.03 | 0.03±0.05 | 0.058 | 0.02±0.04 | 0.04±0.05 | 0.200 | 0.02±0.04 | 0.04±0.09 | 0.881 |
| CIVA (logMAR) | 0.15±0.11 | 0.15±0.08 | 0.691 | 0.08±0.08 | 0.13±0.05 | 0.054 | 0.16±0.09 | 0.16±0.06 | 0.817 |
| CNVA (logMAR) | 0.33±0.11 | 0.32±0.09 | 0.872 | 0.20±0.08 | 0.27±0.10 | 0.040 | 0.28±0.13 | 0.28±0.08 | 0.914 |
Values are presented as mean±standard deviation. Visual acuity is expressed as logarithm of the minimum angle of resolution (logMAR).
PPV, pars plana vitrectomy; SE, spherical equivalent; D, diopter; UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; CIVA, corrected intermediate visual acuity; CNVA, corrected near visual acuity.
a)Advanced monofocal intraocular lens (IOL) group;
b)Hybrid diffractive extended-depth-of-focus (EDoF) IOL group;
c)Hybrid refractive EDoF IOL.
Table 3.Temporal changes in visual acuity within each intraocular lens group
| Group | Time | Δ (95% CI) | P-value |
|---|---|---|---|
| Eyhancea) | |||
| UDVA | Preop to 3 mo | 0.15 (0.05 to 0.25) | 0.005 |
| Preop to 6 mo | 0.14 (0.04 to 0.24) | 0.007 | |
| 3 mo to 6 mo | −0.01 (−0.03 to 0.01) | 0.164 | |
| CDVA | Preop to 3 mo | 0.08 (0.03 to 0.13) | 0.003 |
| Preop to 6 mo | 0.08 (0.03 to 0.13) | 0.003 | |
| 3 mo to 6 mo | NA | ||
| CNVA | Preop to 3 mo | 0.30 (0.15 to 0.46) | 0.001 |
| Preop to 6 mo | 0.30 (0.14 to 0.46) | 0.001 | |
| 3 mo to 6 mo | 0.00 (−0.02 to 0.02) | 0.981 | |
| CIVA | 3 mo to 6 mo | −0.01 (−0.03 to 0.02) | 0.598 |
| Eyhance (PPV) | |||
| UDVA | Preop to 3 mo | 0.51 (0.27 to 0.76) | 0.001 |
| Preop to 6 mo | 0.57 (0.34 to 0.80) | <0.001 | |
| 3 mo to 6 mo | 0.05 (0.00 to 0.11) | 0.061 | |
| CDVA | Preop to 3 mo | 0.35 (0.14 to 0.56) | 0.003 |
| Preop to 6 mo | 0.34 (0.14 to 0.53) | 0.003 | |
| 3 mo to 6 mo | −0.01 (−0.03 to 0.01) | 0.165 | |
| CNVA | Preop to 3 mo | 0.29 (0.13 to 0.45) | 0.002 |
| Preop to 6 mo | 0.30 (0.14 to 0.46) | 0.001 | |
| 3 mo to 6 mo | 0.01 (−0.01 to 0.03) | 0.165 | |
| CIVA | 3 mo to 6 mo | 0.03 (0.00 to 0.06) | 0.040 |
| Symfonyb) | |||
| UDVA | Preop to 3 mo | 0.12 (0.08 to 0.16) | <0.001 |
| Preop to 6 mo | 0.12 (0.07 to 0.17) | <0.001 | |
| 3 mo to 6 mo | 0.00 (−0.03 to 0.03) | 0.974 | |
| CDVA | Preop to 3 mo | 0.10 (0.06 to 0.13) | <0.001 |
| Preop to 6 mo | 0.10 (0.06 to 0.13) | <0.001 | |
| 3 mo to 6 mo | NA | ||
| CNVA | Preop to 3 mo | 0.42 (0.31 to 0.54) | <0.001 |
| Preop to 6 mo | 0.40 (0.28 to 0.51) | <0.001 | |
| 3 mo to 6 mo | −0.02 (−0.07 to 0.02) | 0.271 | |
| CIVA | 3 mo to 6 mo | 0.04 (−0.02 to 0.11) | 0.148 |
| Symfony (PPV) | |||
| UDVA | Preop to 3 mo | 0.46 (0.07 to 0.84) | 0.024 |
| Preop to 6 mo | 0.54 (0.15 to 0.93) | 0.011 | |
| 3 mo to 6 mo | 0.08 (0.05 to 0.11) | <0.001 | |
| CDVA | Preop to 3 mo | 0.05 (0.01 to 0.09) | 0.019 |
| Preop to 6 mo | 0.13 (0.08 to 0.17) | <0.001 | |
| 3 mo to 6 mo | 0.07 (0.05 to 0.10) | <0.001 | |
| CNVA | Preop to 3 mo | 0.20 (0.05 to 0.36) | 0.015 |
| Preop to 6 mo | 0.34 (0.20 to 0.48) | <0.001 | |
| 3 mo to 6 mo | 0.14 (0.08 to 0.20) | <0.001 | |
| CIVA | 3 mo to 6 mo | 0.09 (0.05 to 0.12) | <0.001 |
| Precizonc) | |||
| UDVA | Preop to 3 mo | 0.10 (−0.03 to 0.23) | 0.091 |
| Preop to 6 mo | 0.08 (−0.09 to 0.24) | 0.251 | |
| 3 mo to 6 mo | −0.02 (−0.08 to 0.04) | 0.374 | |
| ΔCDVA | Preop to 3 mo | 0.14 (0.07 to 0.21) | 0.005 |
| Preop to 6 mo | 0.16 (0.05 to 0.27) | 0.017 | |
| 3 mo to 6 mo | 0.02 (−0.03 to 0.07) | 0.374 | |
| ΔCNVA | Preop to 3 mo | 0.24 (−0.06 to 0.54) | 0.086 |
| Preop to 6 mo | 0.24 (−0.06 to 0.54) | 0.086 | |
| 3 mo to 6 mo | 0.00 (−0.09 to 0.09) | >0.999 | |
| ΔCIVA | 3 mo to 6 mo | 0.00 (−0.09 to 0.09) | 0.984 |
| Precizon (PPV) | |||
| UDVA | Preop to 3 mo | 0.08 (−0.10 to 0.27) | 0.294 |
| Preop to 6 mo | 0.14 (−0.10 to 0.38) | 0.181 | |
| 3 mo to 6 mo | 0.06 (−0.01 to 0.13) | 0.071 | |
| CDVA | Preop to 3 mo | 0.05 (−0.03 to 0.12) | 0.180 |
| Preop to 6 mo | 0.12 (0.01 to 0.23) | 0.037 | |
| 3 mo to 6 mo | 0.08 (0.02 to 0.13) | 0.016 | |
| CNVA | Preop to 3 mo | 0.07 (−0.28 to 0.41) | 0.621 |
| Preop to 6 mo | 0.48 (0.26 to 0.70) | 0.004 | |
| 3 mo to 6 mo | 0.41 (0.10 to 0.72) | 0.021 | |
| CIVA | 3 mo to 6 mo | 0.20 (0.11 to 0.29) | 0.003 |
Δ, change between time points; CI, confidence interval; UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; CNVA, corrected near visual acuity; CIVA, corrected intermediate visual acuity; PPV, pars plana vitrectomy; Preop, preoperative; NA, not applicable (standard error of the difference is zero due to identical values).
a)Advanced monofocal intraocular lens (IOL) group;
b)Hybrid diffractive extended-depth-of-focus (EDoF) IOL group;
c)Hybrid refractive EDoF IOL.
Table 4.Comparison of visual outcomes and foveal thickness at 6 months post-surgery among pars plana vitrectomy with epiretinal membrane peeling groups using the Kruskal-Wallis test
- 1. Pedrotti E, Bruni E, Bonacci E, et al. Comparative analysis of the clinical outcomes with a monofocal and an extended range of vision intraocular lens. J Refract Surg 2016;32:436‒42. ArticlePubMed
- 2. Akella SS, Juthani VV. Extended depth of focus intraocular lenses for presbyopia. Curr Opin Ophthalmol 2018;29:318‒22. ArticlePubMed
- 3. Monaco G, Gari M, Di Censo F, et al. Visual performance after bilateral implantation of 2 new presbyopia-correcting intraocular lenses: trifocal versus extended range of vision. J Cataract Refract Surg 2017;43:737‒47. ArticlePubMed
- 4. Mencucci R, Favuzza E, Caporossi O, et al. Comparative analysis of visual outcomes, reading skills, contrast sensitivity, and patient satisfaction with two models of trifocal diffractive intraocular lenses and an extended range of vision intraocular lens. Graefes Arch Clin Exp Ophthalmol 2018;256:1913‒22. ArticlePubMedPDF
- 5. Gundersen KG, Potvin R. Comparing visual acuity, low contrast acuity and contrast sensitivity after trifocal toric and extended depth of focus toric intraocular lens implantation. Clin Ophthalmol 2020;14:1071‒8. ArticlePubMedPMC
- 6. Schmid R, Borkenstein AF. Analysis of higher order aberrations in recently developed wavefront-shaped IOLs. Graefes Arch Clin Exp Ophthalmol 2022;260:609‒20. ArticlePubMedPDF
- 7. Xiao W, Chen X, Yan W, et al. Prevalence and risk factors of epiretinal membranes: a systematic review and meta-analysis of population-based studies. BMJ Open 2017;7:e014644. ArticlePubMedPMC
- 8. Cheung N, Tan SP, Lee SY, et al. Prevalence and risk factors for epiretinal membrane: the Singapore Epidemiology of Eye Disease study. Br J Ophthalmol 2017;101:371‒6. ArticlePubMed
- 9. Mitchell P, Smith W, Chey T, et al. Prevalence and associations of epiretinal membranes: the Blue Mountains Eye Study, Australia. Ophthalmology 1997;104:1033‒40. ArticlePubMed
- 10. Bu SC, Kuijer R, Li XR, et al. Idiopathic epiretinal membrane. Retina 2014;34:2317‒35. ArticlePubMed
- 11. Alio JL, Plaza-Puche AB, Fernandez-Buenaga R, et al. Multifocal intraocular lenses: an overview. Surv Ophthalmol 2017;62:611‒34. ArticlePubMed
- 12. Braga-Mele R, Chang D, Dewey S, et al. Multifocal intraocular lenses: relative indications and contraindications for implantation. J Cataract Refract Surg 2014;40:313‒22. ArticlePubMed
- 13. Jeon S, Choi A, Kwon H. Clinical outcomes after implantation of extended depth-of-focus AcrySof(R) Vivity(R) intraocular lens in eyes with low-grade epiretinal membrane. Graefes Arch Clin Exp Ophthalmol 2022;260:3883‒8. ArticlePubMedPDF
- 14. Chung HS, Lee D, Park JH. Clinical outcomes of combined phacoemulsification, extended depth-of-focus intraocular lens implantation, and epiretinal membrane peeling surgery. J Clin Med 2025;14:2423.ArticlePubMedPMC
- 15. Lee JY, Joo K, Park SJ, et al. Epiretinal membrane surgery in patients with multifocal versus monofocal intraocular lenses. Retina 2021;41:2491‒8. ArticlePubMed
- 16. Yoshino M, Inoue M, Kitamura N, Bissen-Miyajima H. Diffractive multifocal intraocular lens interferes with intraoperative view. Clin Ophthalmol 2010;4:467‒9. ArticlePubMedPMC
- 17. Arrevola-Velasco L, Beltran J, Gimeno MJ, et al. Visual outcomes after vitrectomy for epiretinal membrane in pseudophakic eyes with a diffractive trifocal intraocular lens: a retrospective cohort study. BMC Ophthalmol 2022;22:39.ArticlePubMedPMCPDF
- 18. Inoue M, Aicher NT, Itoh Y, et al. Quality of view through extended depth of focus intraocular lens in a model eye. Jpn J Ophthalmol 2021;65:569‒80. ArticlePubMedPDF
- 19. Photcharapongsakul C, Chokesuwattanaskul S, Choovuthayakorn J, et al. Visual acuity and anatomical changes following vitrectomy for epiretinal membrane foveoschisis: a case series. BMC Ophthalmol 2021;21:433.ArticlePubMedPMCPDF
- 20. Hartmann KI, Schuster AK, Bartsch DU, et al. Restoration of retinal layers after epiretinal membrane peeling. Retina 2014;34:647‒54. ArticlePubMedPMC
- 21. Kokame GT, Tanji TT, Yanagihara RT, et al. Refractive outcomes of combined cataract surgery and vitrectomy compared to cataract surgery alone. Ophthalmologica 2023;246:39‒47. ArticlePubMedPMCPDF
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteClinical outcomes of combined phacoemulsification and epiretinal membrane peeling using three advanced intraocular lens platforms
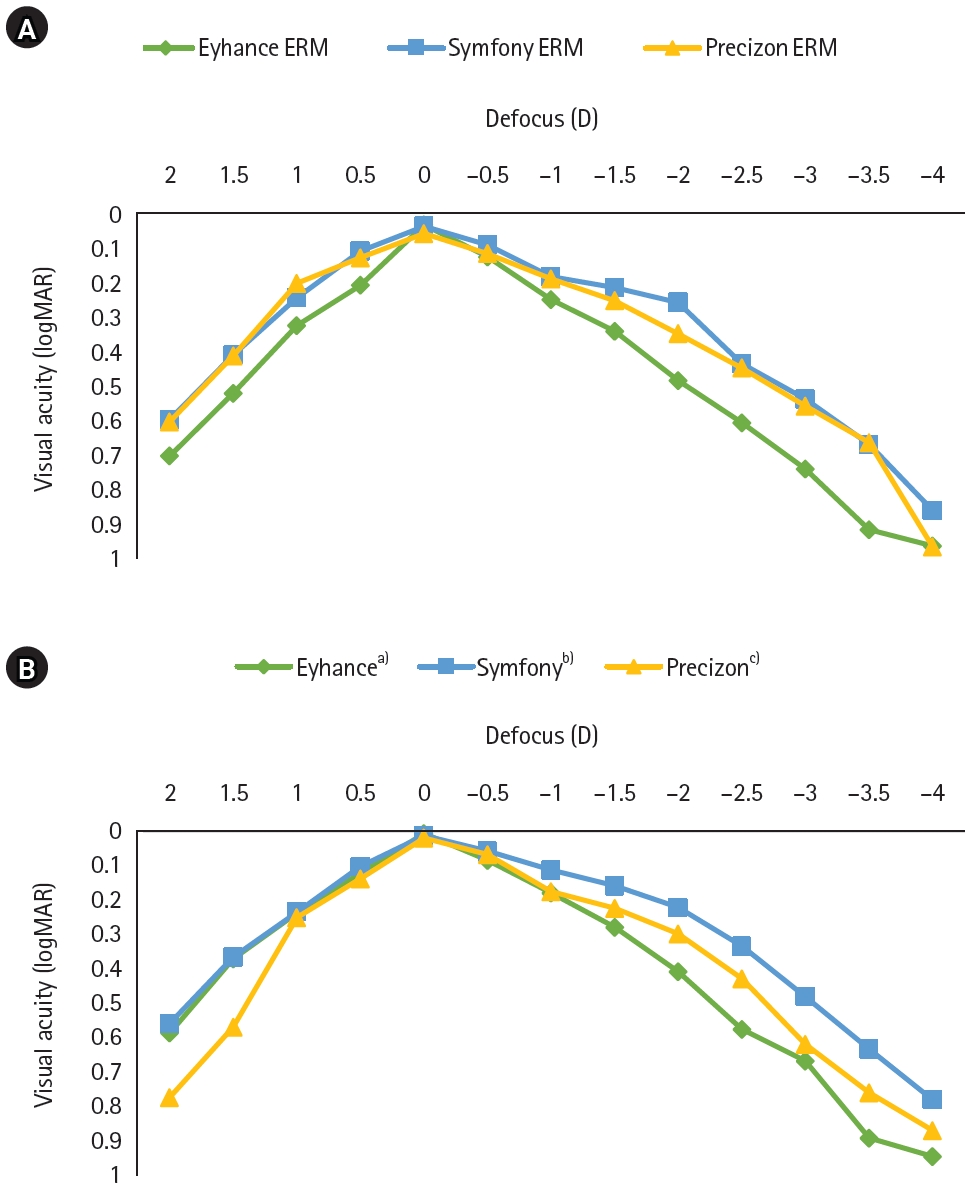
Fig. 1. Defocus curves of the three intraocular lens types at 6 months postoperatively. (A) Eyes that underwent pars plana vitrectomy with epiretinal membrane (ERM) peeling. (B) Control eyes. D, diopter; logMAR, logarithm of the minimum angle of resolution. a)Advanced monofocal intraocular lens (IOL) group; b)Hybrid diffractive extended-depth-of-focus (EDoF) IOL group; c)Hybrid refractive EDoF IOL.
Fig. 1.
Clinical outcomes of combined phacoemulsification and epiretinal membrane peeling using three advanced intraocular lens platforms
| Demographic | Eyhance |
Symfony |
Precizon |
||||||
|---|---|---|---|---|---|---|---|---|---|
| No PPV (n=15) | PPV (n=15) | P-value | No PPV (n=15) | PPV (n=15) | P-value | No PPV (n=5) | PPV (n=5) | P-value | |
| Age (yr) | 68.07±6.18 | 67.93±11.17 | 0.847 | 62.00±6.92 | 60.40±5.60 | 0.487 | 65.00±9.27 | 67.00±5.10 | 0.684 |
| Sex, male/female | 8/7 | 7/8 | 0.726 | 5/10 | 4/11 | 0.787 | 1/4 | 2/3 | 0.545 |
| SE (D) | −0.40±1.81 | −0.18±2.28 | 0.694 | −1.52±4.42 | −1.37±4.20 | 0.781 | −0.85±1.38 | 0.75±0.85 | 0.014 |
| Foveal thickness (µm) | 263.00±18.45 | 360.50±80.82 | <0.001 | 256.31±23.41 | 333.73±61.49 | <0.001 | 273.40±17.42 | 396.00±36.55 | 0.009 |
| UDVA (logMAR) | 0.19±0.18 | 0.64±0.42 | 0.001 | 0.16±0.08 | 0.58±0.71 | <0.001 | 0.18±0.09 | 0.28±0.08 | 0.100 |
| CDVA (logMAR) | 0.09±0.11 | 0.37±0.35 | 0.001 | 0.12±0.06 | 0.16±0.05 | 0.015 | 0.18±0.09 | 0.16±0.06 | 0.911 |
| CNVA (logMAR) | 0.62±0.23 | 0.62±0.25 | 0.733 | 0.60±0.21 | 0.61±0.18 | 0.678 | 0.52±0.18 | 0.76±0.15 | 0.054 |
| Variable | Eyhance |
Symfony |
Precizon |
||||||
|---|---|---|---|---|---|---|---|---|---|
| No PPV (n=15) | PPV (n=15) | P-value | No PPV (n=15) | PPV (n=15) | P-value | No PPV (n=5) | PPV (n=5) | P-value | |
| Postoperative 3 mo | |||||||||
| SE (D) | −0.07±0.54 | −0.13±0.52 | 0.824 | −0.39±0.46 | −0.40±0.66 | 0.614 | −1.15±0.82 | −0.80±0.87 | 0.343 |
| Foveal thickness (µm) | 268.27±19.52 | 354.29±70.82 | <0.001 | 258.38±23.29 | 325.87±56.49 | <0.001 | 270.40±13.47 | 379.80±29.74 | 0.009 |
| UDVA (logMAR) | 0.03±0.04 | 0.13±0.11 | 0.004 | 0.04±0.05 | 0.13±0.07 | 0.002 | 0.08±0.08 | 0.20±0.07 | 0.049 |
| CDVA (logMAR) | 0.01±0.03 | 0.02±0.04 | 0.258 | 0.02±0.04 | 0.11±0.06 | <0.001 | 0.04±0.05 | 0.12±0.05 | 0.042 |
| CIVA (logMAR) | 0.14±0.09 | 0.18±0.08 | 0.186 | 0.12±0.09 | 0.22±0.09 | 0.009 | 0.16±0.06 | 0.36±0.05 | 0.007 |
| CNVA (logMAR) | 0.33±0.12 | 0.33±0.11 | 0.891 | 0.17±0.08 | 0.41±0.15 | <0.001 | 0.28±0.15 | 0.69±0.18 | 0.013 |
| Postoperative 6 mo | |||||||||
| SE (D) | −0.10±0.43 | −0.14±0.48 | 0.532 | −0.38±0.46 | −0.38±0.57 | 0.791 | −1.15±0.80 | −0.65±0.68 | 0.292 |
| Foveal thickness (µm) | 262.87±17.80 | 339.07±73.90 | <0.001 | 260.19±20.93 | 311.47±49.84 | <0.001 | 271.80±16.22 | 347.00±27.15 | 0.009 |
| UDVA (logMAR) | 0.04±0.05 | 0.07±0.10 | 0.422 | 0.04±0.06 | 0.05±0.06 | 0.890 | 0.10±0.10 | 0.14±0.11 | 0.588 |
| CDVA (logMAR) | 0.01±0.03 | 0.03±0.05 | 0.058 | 0.02±0.04 | 0.04±0.05 | 0.200 | 0.02±0.04 | 0.04±0.09 | 0.881 |
| CIVA (logMAR) | 0.15±0.11 | 0.15±0.08 | 0.691 | 0.08±0.08 | 0.13±0.05 | 0.054 | 0.16±0.09 | 0.16±0.06 | 0.817 |
| CNVA (logMAR) | 0.33±0.11 | 0.32±0.09 | 0.872 | 0.20±0.08 | 0.27±0.10 | 0.040 | 0.28±0.13 | 0.28±0.08 | 0.914 |
| Group | Time | Δ (95% CI) | P-value |
|---|---|---|---|
| Eyhance |
|||
| UDVA | Preop to 3 mo | 0.15 (0.05 to 0.25) | 0.005 |
| Preop to 6 mo | 0.14 (0.04 to 0.24) | 0.007 | |
| 3 mo to 6 mo | −0.01 (−0.03 to 0.01) | 0.164 | |
| CDVA | Preop to 3 mo | 0.08 (0.03 to 0.13) | 0.003 |
| Preop to 6 mo | 0.08 (0.03 to 0.13) | 0.003 | |
| 3 mo to 6 mo | NA | ||
| CNVA | Preop to 3 mo | 0.30 (0.15 to 0.46) | 0.001 |
| Preop to 6 mo | 0.30 (0.14 to 0.46) | 0.001 | |
| 3 mo to 6 mo | 0.00 (−0.02 to 0.02) | 0.981 | |
| CIVA | 3 mo to 6 mo | −0.01 (−0.03 to 0.02) | 0.598 |
| Eyhance (PPV) | |||
| UDVA | Preop to 3 mo | 0.51 (0.27 to 0.76) | 0.001 |
| Preop to 6 mo | 0.57 (0.34 to 0.80) | <0.001 | |
| 3 mo to 6 mo | 0.05 (0.00 to 0.11) | 0.061 | |
| CDVA | Preop to 3 mo | 0.35 (0.14 to 0.56) | 0.003 |
| Preop to 6 mo | 0.34 (0.14 to 0.53) | 0.003 | |
| 3 mo to 6 mo | −0.01 (−0.03 to 0.01) | 0.165 | |
| CNVA | Preop to 3 mo | 0.29 (0.13 to 0.45) | 0.002 |
| Preop to 6 mo | 0.30 (0.14 to 0.46) | 0.001 | |
| 3 mo to 6 mo | 0.01 (−0.01 to 0.03) | 0.165 | |
| CIVA | 3 mo to 6 mo | 0.03 (0.00 to 0.06) | 0.040 |
| Symfony |
|||
| UDVA | Preop to 3 mo | 0.12 (0.08 to 0.16) | <0.001 |
| Preop to 6 mo | 0.12 (0.07 to 0.17) | <0.001 | |
| 3 mo to 6 mo | 0.00 (−0.03 to 0.03) | 0.974 | |
| CDVA | Preop to 3 mo | 0.10 (0.06 to 0.13) | <0.001 |
| Preop to 6 mo | 0.10 (0.06 to 0.13) | <0.001 | |
| 3 mo to 6 mo | NA | ||
| CNVA | Preop to 3 mo | 0.42 (0.31 to 0.54) | <0.001 |
| Preop to 6 mo | 0.40 (0.28 to 0.51) | <0.001 | |
| 3 mo to 6 mo | −0.02 (−0.07 to 0.02) | 0.271 | |
| CIVA | 3 mo to 6 mo | 0.04 (−0.02 to 0.11) | 0.148 |
| Symfony (PPV) | |||
| UDVA | Preop to 3 mo | 0.46 (0.07 to 0.84) | 0.024 |
| Preop to 6 mo | 0.54 (0.15 to 0.93) | 0.011 | |
| 3 mo to 6 mo | 0.08 (0.05 to 0.11) | <0.001 | |
| CDVA | Preop to 3 mo | 0.05 (0.01 to 0.09) | 0.019 |
| Preop to 6 mo | 0.13 (0.08 to 0.17) | <0.001 | |
| 3 mo to 6 mo | 0.07 (0.05 to 0.10) | <0.001 | |
| CNVA | Preop to 3 mo | 0.20 (0.05 to 0.36) | 0.015 |
| Preop to 6 mo | 0.34 (0.20 to 0.48) | <0.001 | |
| 3 mo to 6 mo | 0.14 (0.08 to 0.20) | <0.001 | |
| CIVA | 3 mo to 6 mo | 0.09 (0.05 to 0.12) | <0.001 |
| Precizon |
|||
| UDVA | Preop to 3 mo | 0.10 (−0.03 to 0.23) | 0.091 |
| Preop to 6 mo | 0.08 (−0.09 to 0.24) | 0.251 | |
| 3 mo to 6 mo | −0.02 (−0.08 to 0.04) | 0.374 | |
| ΔCDVA | Preop to 3 mo | 0.14 (0.07 to 0.21) | 0.005 |
| Preop to 6 mo | 0.16 (0.05 to 0.27) | 0.017 | |
| 3 mo to 6 mo | 0.02 (−0.03 to 0.07) | 0.374 | |
| ΔCNVA | Preop to 3 mo | 0.24 (−0.06 to 0.54) | 0.086 |
| Preop to 6 mo | 0.24 (−0.06 to 0.54) | 0.086 | |
| 3 mo to 6 mo | 0.00 (−0.09 to 0.09) | >0.999 | |
| ΔCIVA | 3 mo to 6 mo | 0.00 (−0.09 to 0.09) | 0.984 |
| Precizon (PPV) | |||
| UDVA | Preop to 3 mo | 0.08 (−0.10 to 0.27) | 0.294 |
| Preop to 6 mo | 0.14 (−0.10 to 0.38) | 0.181 | |
| 3 mo to 6 mo | 0.06 (−0.01 to 0.13) | 0.071 | |
| CDVA | Preop to 3 mo | 0.05 (−0.03 to 0.12) | 0.180 |
| Preop to 6 mo | 0.12 (0.01 to 0.23) | 0.037 | |
| 3 mo to 6 mo | 0.08 (0.02 to 0.13) | 0.016 | |
| CNVA | Preop to 3 mo | 0.07 (−0.28 to 0.41) | 0.621 |
| Preop to 6 mo | 0.48 (0.26 to 0.70) | 0.004 | |
| 3 mo to 6 mo | 0.41 (0.10 to 0.72) | 0.021 | |
| CIVA | 3 mo to 6 mo | 0.20 (0.11 to 0.29) | 0.003 |
| Outcome | χ2 | P-value |
|---|---|---|
| Uncorrected distance visual acuity | 3.395 | 0.183 |
| Corrected distance visual acuity | 0.244 | 0.885 |
| Corrected intermediate visual acuity | 1.105 | 0.575 |
| Corrected near visual acuity | 2.356 | 0.308 |
| Foveal thickness | 2.879 | 0.237 |
Table 1. Demographics and preoperative clinical characteristics of the study patients at baseline
Values are presented as mean±standard deviation. Visual acuity is expressed as logarithm of the minimum angle of resolution (logMAR). PPV, pars plana vitrectomy; SE, spherical equivalent; D, diopter; UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; CNVA, corrected near visual acuity. Advanced monofocal intraocular lens (IOL) group; Hybrid diffractive extended-depth-of-focus (EDoF) IOL group; Hybrid refractive EDoF IOL.
Table 2. Postoperative visual acuity, refraction, and foveal thickness compared with controls
Values are presented as mean±standard deviation. Visual acuity is expressed as logarithm of the minimum angle of resolution (logMAR). PPV, pars plana vitrectomy; SE, spherical equivalent; D, diopter; UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; CIVA, corrected intermediate visual acuity; CNVA, corrected near visual acuity. Advanced monofocal intraocular lens (IOL) group; Hybrid diffractive extended-depth-of-focus (EDoF) IOL group; Hybrid refractive EDoF IOL.
Table 3. Temporal changes in visual acuity within each intraocular lens group
Δ, change between time points; CI, confidence interval; UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; CNVA, corrected near visual acuity; CIVA, corrected intermediate visual acuity; PPV, pars plana vitrectomy; Preop, preoperative; NA, not applicable (standard error of the difference is zero due to identical values). Advanced monofocal intraocular lens (IOL) group; Hybrid diffractive extended-depth-of-focus (EDoF) IOL group; Hybrid refractive EDoF IOL.
Table 4. Comparison of visual outcomes and foveal thickness at 6 months post-surgery among pars plana vitrectomy with epiretinal membrane peeling groups using the Kruskal-Wallis test

