
Articles
- Page Path
- HOME > Insights Cataract Refract Surg > Volume 10(3); 2025 > Article
-
Original Article
각막굴절교정수술을 받은 환자에서 다초점 인공수정체 삽입 결과 -
김은철

-
Results of multifocal intraocular lens implantation in patients who underwent corneal refractive surgery -
Eun Chul Kim
-
Insights in Cataract and Refractive Surgery 2025;10(3):76-82.
DOI: https://doi.org/10.63375/icrs.25.011
Published online: October 31, 2025
가톨릭대학교 의과대학 부천성모병원 안과학교실
Department of Ophthalmology, Bucheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- Correspondence: Eun Chul Kim Department of Ophthalmology, The Catholic University of Korea, Bucheon St. Mary's Hospital, 327 Sosa-ro, Wonmi-gu, Bucheon 14647, Korea Tel: +82-32-340-2125 E-mail: eunchol@hanmail.net
• Received: August 12, 2025 • Revised: September 26, 2025 • Accepted: September 27, 2025
© 2025 Korean Society of Cataract and Refractive Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 911 Views
- 14 Download
국문초록
-
목적
- 각막굴절교정수술을 받은 백내장 환자에서 삼중초점 인공수정체의 임상 결과를 알아보고자 한다.
-
방법
- 과거에 각막굴절교정수술을 받은 환자에서 삼중초점 인공수정체(Synergy: ZFR00V)를 삽입한 30안(16명)을 대상으로 후향적으로 연구하였다. 술 후 1, 3개월 나안과 교정 원거리, 중간 거리, 근거리 시력과 현성굴절검사 및 환자만족도 설문을 시행하였다.
-
결과
- 삼중초점 인공수정체 삽입 후 나안 원거리, 중간 거리, 근거리 시력과 현성굴절검사는 각각 수술 전보다 개선되었다(P<0.05). 수술 후 굴절값과 인공수정체 계산값의 오차는 Haigis-L보다 Barret True K 공식이 더 적었다(P<0.05). 탈초점 곡선상 0 diopter (D)뿐만 아니라 –1에서 –1.5 D까지와 –2.5에서 –4.0 D까지 곡선의 상승이 있어 원거리, 중간 거리, 근거리의 시력 개선이 있었다. 설문 조사에서 원거리 만족도(1.47±0.63), 근거리 만족도(1.25±0.71)와 전반적 만족도(1.36±0.42)는 좋았으나 빛 번짐과 달무리 만족도(1.97±0.85)는 좋지 않았다.
-
결론
- 과거 각막굴절교정수술을 받은 백내장 환자에서 다초점 인공수정체를 삽입한 결과, 원거리, 중간 거리, 근거리 나안 시력이 우수하였으나 빛 번짐과 달무리의 부작용이 있었으므로 환자 선택에 신중을 가해야 할 것이다.
Abstract
-
Purpose
- The aim of this study was to evaluate the clinical results of multifocal intraocular lenses in patients who underwent corneal refractive surgery.
-
Methods
- Thirty eyes (16 patients; Synergy: ZFR00V) were retrospectively enrolled. Uncorrected and corrected near visual acuity (UNVA, CNVA), intermediate visual acuity (UIVA, CIVA), and distant visual acuity (UDVA, CDVA), manifest refraction spherical equivalent (MRSE), and satisfaction score were assessed before and after surgery.
-
Results
- The postoperative UDVA, UIVA, UNVA, and MRSE of the three groups exhibited improvements compared to the preoperative data (P<0.05). The error between the postoperative refraction and the intraocular lens calculation was smaller with the Barrett True K formula than with the Haigis-L formula (P<0.05). The defocus curve at 0 diopter (D) increased, from –1 to –1.5 D, and from –2.5 to –4.0 D, indicating improved vision at distant, intermediate, and near distances. Distance satisfaction (1.47±0.63), near satisfaction (1.25±0.71), and overall satisfaction (1.36±0.42) were good, but light scattering and halo satisfaction (1.97±0.85) yielded a poor result.
-
Conclusion
- In patients with cataracts who underwent corneal refractive surgery, multifocal intraocular lens implantation resulted in excellent uncorrected visual acuity at distant, intermediate, and near distances. However, careful consideration should be given to patient selection due to the incidence of side effects such as glare and halos.
서론
방법
결과
고찰
Article Information
Author contributions
All the work was done by ECK.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
Not applicable.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Fig. 1.Percentage of eyes within target refraction. The postoperative percentage of eyes within ±0.50 D was 73.3% and ±1.0 D was 90.0%.
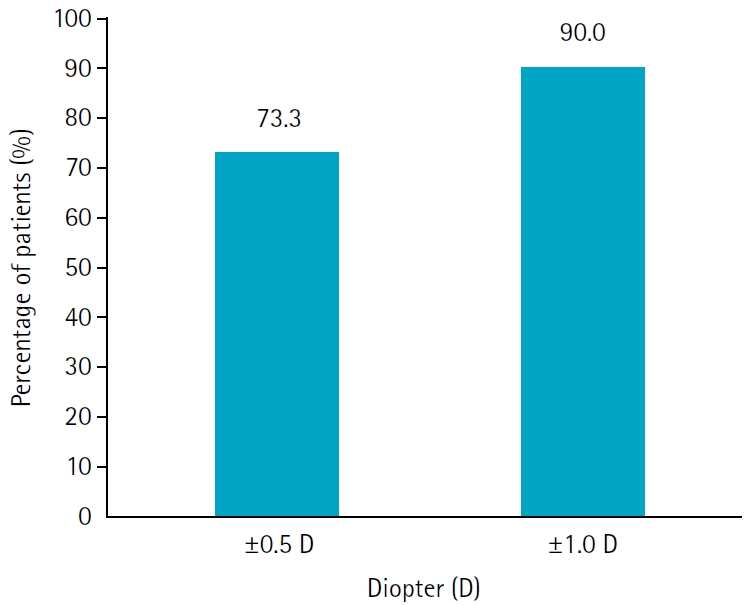
Fig. 2.Mean defocus curves. The defocus curve showed a peak at defocus 0 D (4 m) and a smooth curve along the intermediate distance range (–1.5 to –2 D; corresponding to 50 to 67 cm), and good visual acuity results were also observed at the defocus curve of –3 D (corresponding to 33 cm). LogMAR, logarithm of the minimum angle of resolution.
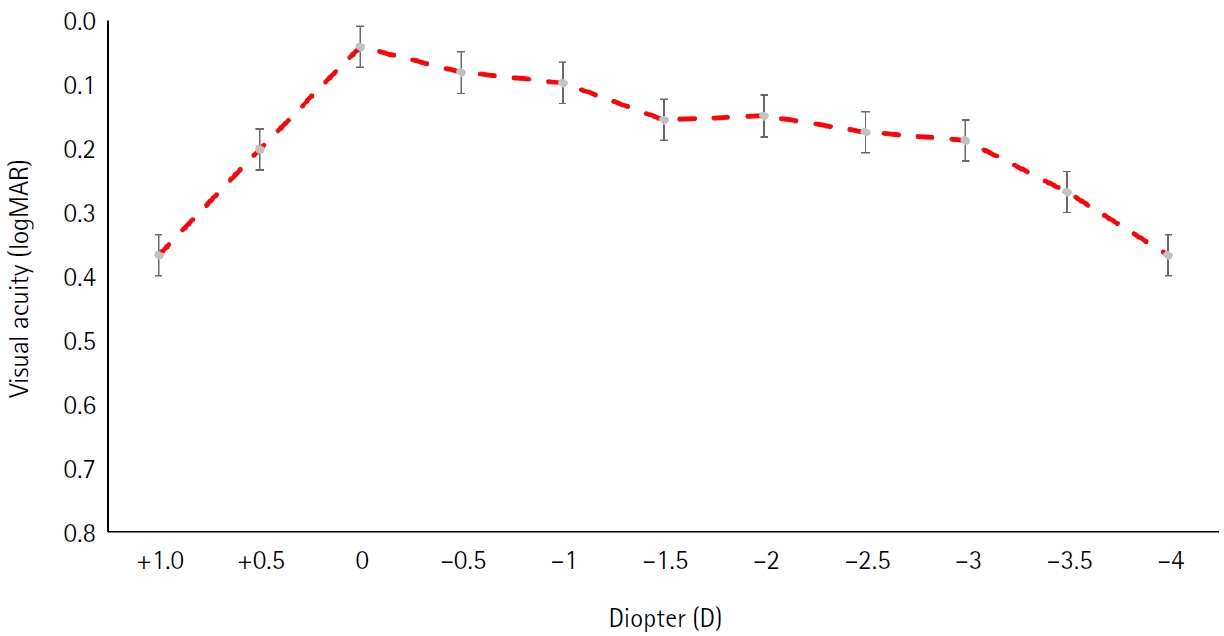
Table 1.Preoperative data
Table 2.Postoperative outcomes at 2 months after surgery
| Parameter | Value |
|---|---|
| Postoperative UDVA (logMAR) | 0.05±0.02 |
| Postoperative CDVA (logMAR) | 0.02±0.01 |
| Postoperative UIVA (logMAR) | 0.04±0.02 |
| Postoperative UNVA (logMAR) | 0.03±0.01 |
| Manifest sphere (D) | –0.11±0.21 |
| Manifest cylinder (D) | –0.58±0.28 |
| Manifest spherical equivalent (D) | –0.4±0.32 |
| Target refraction of Haigis-L (D) | 0.18±0.32 (P=0.04)* |
| Target refraction of Barrett True-K (D) | 0.10±0.25 (P>0.05) |
| No. of eyes | 30 |
Values are presented as mean±standard deviation. The Haigis-L was significantly different from postoperative manifest spherical equivalent refraction.
UDVA, uncorrected distant visual acuity; CDVA, corrected distant visual acuity; UIVA, uncorrected intermediate visual acuity; UNVA, uncorrected near visual acuity; logMAR, logarithm of the minimum angle of resolution; D, diopter.
*P<0.05.
Table 3.Subjective satisfaction score
| Parameter | Value |
|---|---|
| Overall satisfaction | 1.36±0.42 |
| Far vision satisfaction | 1.47±0.63 |
| Near vision satisfaction | 1.25±0.71 |
| Glare, Halo | 1.97±0.85* |
| No. of eyes | 30 |
- 1. Moshirfar M, Ostler EM, Smedley JG, et al. Age of cataract extraction in post-refractive surgery patients. J Cataract Refract Surg 2014;40:841‒2. ArticlePubMed
- 2. Brierley L. Refractive results after implantation of a light-adjustable intraocular lens in postrefractive surgery cataract patients. Ophthalmology 2013;120:1968‒72. ArticlePubMed
- 3. Wang SY, Stem MS, Oren G, et al. Patient-centered and visual quality outcomes of premium cataract surgery: a systematic review. Eur J Ophthalmol 2017;27:387‒401. ArticlePubMedPDF
- 4. Khandelwal SS, Jun JJ, Mak S, et al. Effectiveness of multifocal and monofocal intraocular lenses for cataract surgery and lens replacement: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol 2019;257:863‒75. ArticlePubMedPDF
- 5. Alio JL, Alio Del Barrio JL, Vega-Estrada A. Accommodative intraocular lenses: where are we and where we are going. Eye Vis (Lond) 2017;4:16.ArticlePubMedPMC
- 6. Wang L, Koch DD. Intraocular lens power calculations in eyes with previous corneal refractive surgery: review and expert opinion. Ophthalmology 2021;128:e121‒31. ArticlePubMed
- 7. Cochener B. Clinical outcomes of a new extended range of vision intraocular lens: international multicenter concerto study. J Cataract Refract Surg 2016;42:1268‒75. ArticlePubMed
- 8. Bilbao-Calabuig R, Ortega-Usobiaga J, Mayordomo-Cerda F, et al. Trifocal versus monofocal intraocular lens implantation in eyes previously treated with laser in situ keratomileusis (LASIK) for myopia. Indian J Ophthalmol 2024;72(Suppl 2):S254‒9. ArticlePubMedPMC
- 9. Bai G, Li X, Zhang S, et al. Analysis of visual quality after multifocal intraocular lens implantation in post-LASIK cataract patients. Heliyon 2023;9:e15720. ArticlePubMedPMC
- 10. Saiki M, Negishi K, Kato N, et al. Ray tracing software for intraocular lens power calculation after corneal excimer laser surgery. Jpn J Ophthalmol 2014;58:276‒81. ArticlePubMedPDF
- 11. Wang L, Tang M, Huang D, et al. Comparison of newer intraocular lens power calculation methods for eyes after corneal refractive surgery. Ophthalmology 2015;122:2443‒9. ArticlePubMedPMC
- 12. Chan TC, Liu D, Yu M, Jhanji V. Longitudinal evaluation of posterior corneal elevation after laser refractive surgery using swept-source optical coherence tomography. Ophthalmology 2015;122:687‒92. ArticlePubMed
- 13. Lwowski C, Pawlowicz K, Hinzelmann L, et al. Prediction accuracy of IOL calculation formulas using the ASCRS online calculator for a diffractive extended depth-of-focus IOL after myopic laser in situ keratomileusis. J Cataract Refract Surg 2020;46:1240‒6. ArticlePubMed
- 14. Tan Q, Wang Y, Zhao L, et al. Prediction accuracy of no-history intraocular lens formulas for a diffractive extended depth-of-focus intraocular lens after myopic corneal refractive surgery. J Cataract Refract Surg 2022;48:462‒8. ArticlePubMed
- 15. Lwowski C, Van Keer K, Adas M, et al. Ray-tracing calculation using scheimpflug tomography of diffractive extended depth of focus IOLs following myopic LASIK. J Refract Surg 2021;37:231‒9. ArticlePubMed
- 16. Carreras H, Renones J, Carreras MD, et al. Clinical performance of an extended range of vision intraocular lens after LASIK. J Refract Surg 2024;40:e742‒53. ArticlePubMed
- 17. Chow SS, Chan TC, Ng AL, Kwok AK. Outcomes of presbyopia-correcting intraocular lenses after laser in situ keratomileusis. Int Ophthalmol 2019;39:1199‒204. ArticlePubMedPDF
- 18. Vrijman V, van der Linden JW, van der Meulen IJ, et al. Multifocal intraocular lens implantation after previous corneal refractive laser surgery for myopia. J Cataract Refract Surg 2017;43:909‒14. ArticlePubMed
- 19. Vryghem JC, Laouani A, Mansouri M. Clinical outcomes using a trifocal intraocular lens in eyes after previous laser corneal refractive surgery or radial keratotomy: 1-year of follow-up. Clin Ophthalmol 2025;19:3089‒102. ArticlePubMedPMCPDF
- 20. Susanna BN, Ferguson TJ, Randleman JB. Cataract surgery following refractive surgery: principles for success. Asia Pac J Ophthalmol (Phila) 2025;14:100227.ArticlePubMed
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteResults of multifocal intraocular lens implantation in patients who underwent corneal refractive surgery
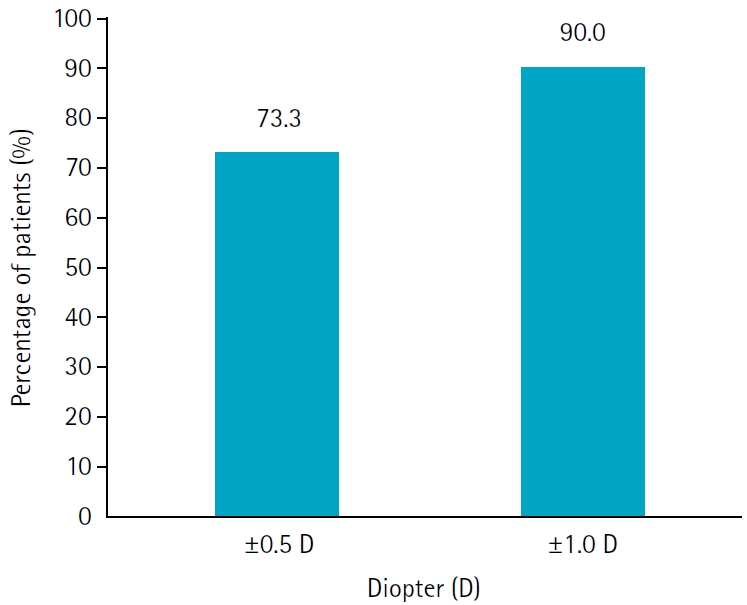
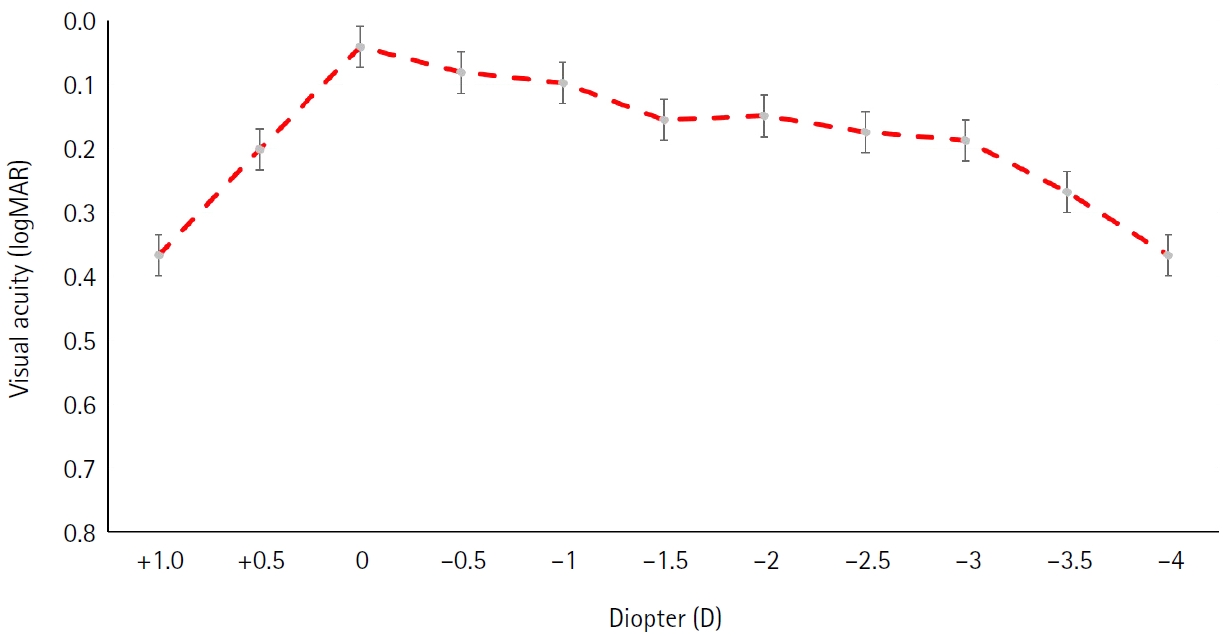
Fig. 1. Percentage of eyes within target refraction. The postoperative percentage of eyes within ±0.50 D was 73.3% and ±1.0 D was 90.0%.
Fig. 2. Mean defocus curves. The defocus curve showed a peak at defocus 0 D (4 m) and a smooth curve along the intermediate distance range (–1.5 to –2 D; corresponding to 50 to 67 cm), and good visual acuity results were also observed at the defocus curve of –3 D (corresponding to 33 cm). LogMAR, logarithm of the minimum angle of resolution.
Fig. 1.
Fig. 2.
Results of multifocal intraocular lens implantation in patients who underwent corneal refractive surgery
| Parameter | Value |
|---|---|
| OD:OS | 15:15 |
| Sex (male:female) | 6:10 |
| Age (yr) | 60.1±6.2 (50 to 75) |
| Preoperative UDVA (logMAR) | 0.35±0.21 (0.12 to 0.67) |
| Preoperative CDVA (logMAR) | 0.23±0.15 (0.10 to 0.53) |
| Manifest sphere (D) | 1.68±1.98 (–3.50 to 4.50) |
| Manifest cylinder (D) | –1.25±0.74 (–2.50 to 0.00) |
| Manifest spherical equivalent (D) | 1.57±2.35 (–3.25 to 4.25) |
| Intraocular lens power (D) | 19.54±1.78 (15.5 to 23.0) |
| No. of eyes | 30 |
| Parameter | Value |
|---|---|
| Postoperative UDVA (logMAR) | 0.05±0.02 |
| Postoperative CDVA (logMAR) | 0.02±0.01 |
| Postoperative UIVA (logMAR) | 0.04±0.02 |
| Postoperative UNVA (logMAR) | 0.03±0.01 |
| Manifest sphere (D) | –0.11±0.21 |
| Manifest cylinder (D) | –0.58±0.28 |
| Manifest spherical equivalent (D) | –0.4±0.32 |
| Target refraction of Haigis-L (D) | 0.18±0.32 (P=0.04) |
| Target refraction of Barrett True-K (D) | 0.10±0.25 (P>0.05) |
| No. of eyes | 30 |
| Parameter | Value |
|---|---|
| Overall satisfaction | 1.36±0.42 |
| Far vision satisfaction | 1.47±0.63 |
| Near vision satisfaction | 1.25±0.71 |
| Glare, Halo | 1.97±0.85 |
| No. of eyes | 30 |
Table 1. Preoperative data
Values are presented as mean±standard deviation (range). OD, oculus dexter; OS, oculus sinister; UDVA, uncorrected distant visual acuity; CDVA, corrected distant visual acuity; logMAR, logarithm of the minimum angle of resolution; D, diopter.
Table 2. Postoperative outcomes at 2 months after surgery
Values are presented as mean±standard deviation. The Haigis-L was significantly different from postoperative manifest spherical equivalent refraction. UDVA, uncorrected distant visual acuity; CDVA, corrected distant visual acuity; UIVA, uncorrected intermediate visual acuity; UNVA, uncorrected near visual acuity; logMAR, logarithm of the minimum angle of resolution; D, diopter. P<0.05.
Table 3. Subjective satisfaction score
Values are presented as mean±standard deviation. A low score indicates high satisfaction. Glare and halo satisfaction was significantly lower than the overall, far vision, or near vision satisfaction, respectively. P<0.05.

