
Articles
- Page Path
- HOME > Insights Cataract Refract Surg > Volume 11(1); 2026 > Article
-
Original Article
- Impact of anterior chamber depth to axial length ratio on conventional intraocular lens power calculation formulas performance in axial myopia
-
Youngsub Eom1,#
 , Jinhwan Park2, Youngbin Song2, Dong Hyun Kim1, Jong Suk Song1
, Jinhwan Park2, Youngbin Song2, Dong Hyun Kim1, Jong Suk Song1 -
Insights in Cataract and Refractive Surgery 2026;11(1):15-22.
DOI: https://doi.org/10.63375/icrs.25.017
Published online: February 26, 2026
1Department of Ophthalmology, Korea University College of Medicine, Seoul, Korea
2YES Eye Clinic, Seoul, Korea
- Correspondence to: Youngsub Eom YES Eye Clinic, 32 Deungchon-ro, Yangcheon-gu, Seoul 07965, Korea Tel: +82-2-6956-1112 E-mail: hippotate@hanmail.net
- #Current affiliation: YES Eye Clinic, Seoul, Korea
• Received: December 25, 2025 • Revised: January 13, 2026 • Accepted: January 14, 2026
© 2026 Korean Society of Cataract and Refractive Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 588 Views
- 7 Download
Abstract
-
Purpose
- To evaluate the effects of the ratio of anterior chamber depth to axial length (ACD/AL), as well as axial length (AL) itself, on the accuracy of conventional intraocular lens (IOL) power calculation formulas in eyes with axial myopia.
-
Methods
- This retrospective cross-sectional study included 60 eyes from 44 patients with an AL greater than 25.0 mm who underwent uncomplicated phacoemulsification with IOL implantation. Eyes were categorized into high and low AL groups using an AL threshold of 27.0 mm, and into high and low ACD/AL groups based on the median ACD/AL value of 13.4. The median absolute errors (MedAEs) predicted by the Sanders-Retzlaff-Kraff theoretical (SRK/T) and Haigis formulas were compared according to AL and ACD/AL groupings.
-
Results
- In the low ACD/AL group and in the high AL group, the MedAEs predicted by the Haigis formula were lower than those predicted by the SRK/T formula (P=0.002 and P=0.012, respectively). The MedAEs predicted by both the SRK/T and Haigis formulas were significantly lower in the high ACD/AL group than in the low ACD/AL group (P<0.001 and P=0.010, respectively). In contrast, no significant difference was observed between the low and high AL groups in the MedAEs predicted by the Haigis formula. When the ACD/AL ratio was less than 13.4, postoperative refractive outcomes were more hyperopic with both formulas.
-
Conclusion
- In eyes with a long AL and a relatively shallow ACD, the Haigis formula demonstrated superior accuracy among conventional IOL power calculation formulas. Under these anatomical conditions, targeting slightly more myopic postoperative refractions may therefore be advisable.
Introduction
Methods
Results
Discussion
Article Information
Author contributions
Conceptualization: YE, JSS. Formal analysis: all authors. Investigation: all authors. Methodology: YE, DHK, JSS. Supervision: YE, JSS. Writing – original draft: YE. Writing – review & editing: all authors. Final approval of the manuscript: all authors.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Acknowledgments
We sincerely thank Dr. Yong Yeon Kim (Kim’s Eye Hospital, Seoul, Korea) for performing cataract surgeries and contributing to the clinical care of the patients whose medical records were used in this retrospective study.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Fig. 1.Linear regression analysis illustrating the relationships among anterior chamber depth (ACD), axial length (AL), the ACD to AL ratio (ACD/AL), and the absolute value of the predicted refractive error calculated using the Sanders-Retzlaff-Kraff theoretical (SRK/T) and Haigis formulas. Panels A–C present the associations for the SRK/T formula with ACD (A), AL (B), and ACD/AL (C), whereas panels D–F depict the corresponding associations for the Haigis formula with ACD (D), AL (E), and ACD/AL (F). MAE, mean absolute error; D, diopters.
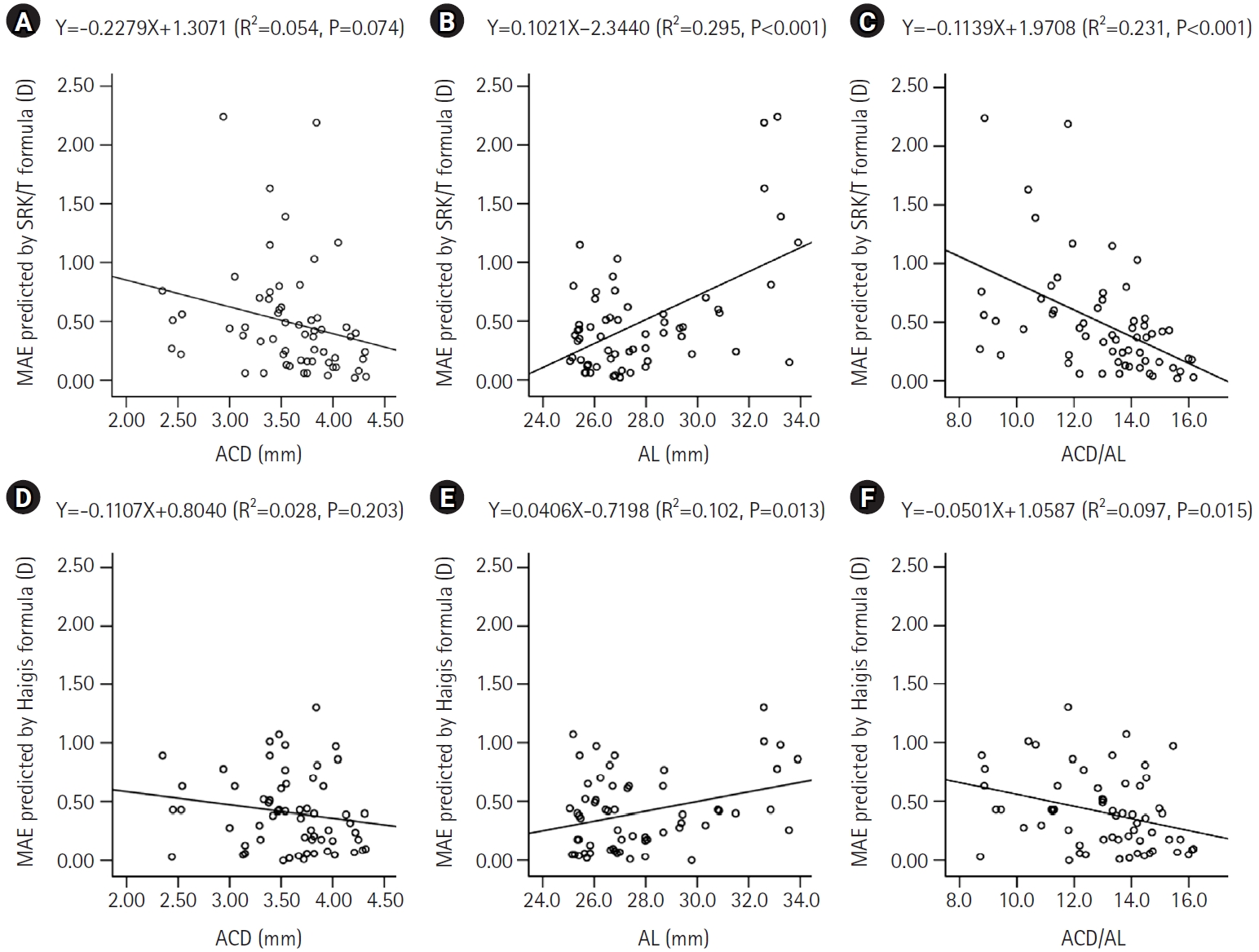
Fig. 2.Comparison of the predicted refractive error according to the anterior chamber depth to axial length ratio (ACD/AL) using the Sanders-Retzlaff-Kraff theoretical formula (A) and the Haigis formula (B). D, diopters.
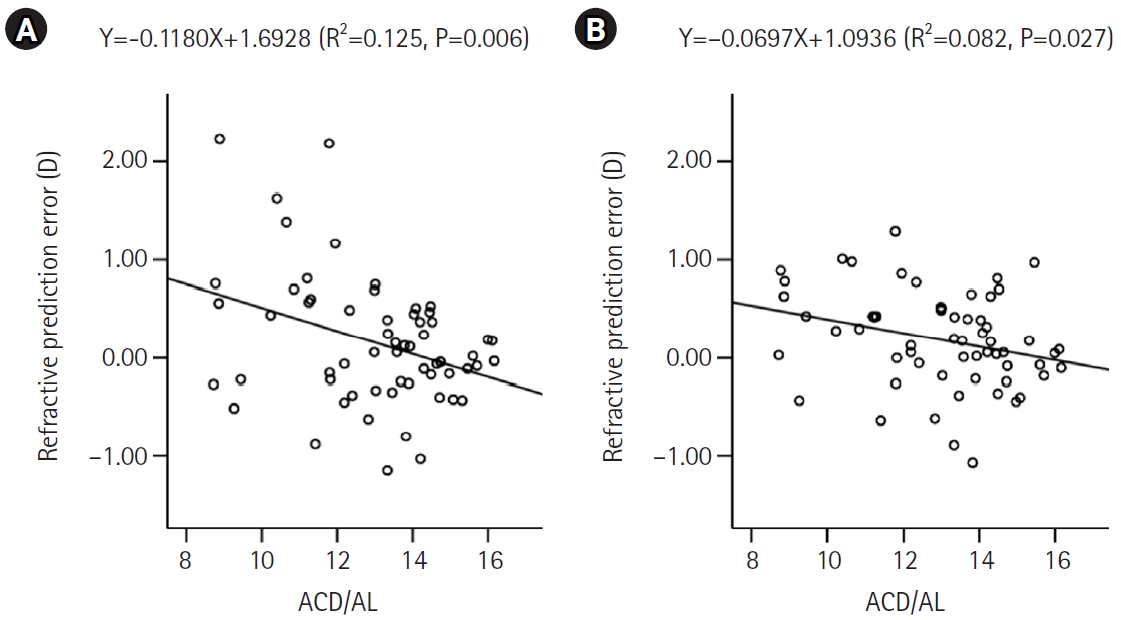
Fig. 3.Graph depicting the theoretical ratio of ACD/AL across varying AL, generated after setting the corneal power to 44.4 diopters, corresponding to the mean corneal power in this study, using the Sanders-Retzlaff-Kraff theoretical formula. ACD/AL, anterior chamber depth to axial length ratio.
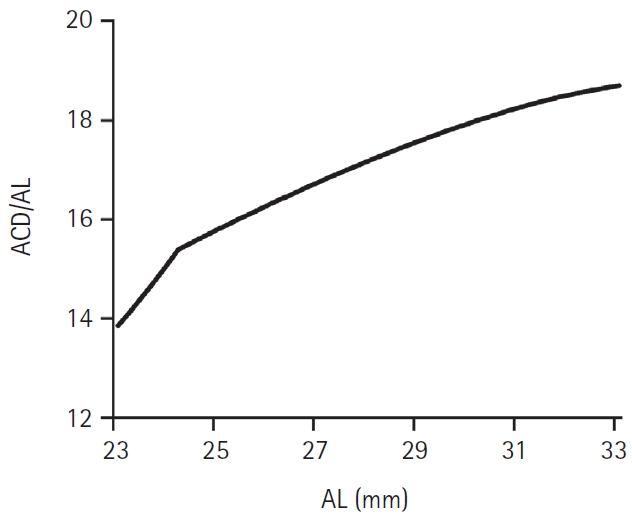
Table 1.The clinical and demographic characteristics of the subjects included in the present study (n=60)
| Demographic | Value |
|---|---|
| Age (yr) | 59.6±13.5 (16–83) |
| Sexa) | |
| Male | 16 (36.4) |
| Female | 28 (63.6) |
| Lateralitya) | |
| Right eye | 34 (56.7) |
| Left eye | 26 (43.3) |
| Corneal power (D) | 44.43±1.50 (41.57 to 48.49) |
| Anterior chamber depth (mm) | 3.58±0.48 (2.35 to 4.32) |
| Axial length (mm) | 27.76±2.51 (25.05 to 33.90) |
| IOL power (D) | 9.2±6.7 (–7.0 to 18.0) |
Table 2.MedAE and MAE as predicted by different formulas
| Formula | Whole subjects (n=60) | P-valuea) | ||
|---|---|---|---|---|
| MedAE (D) | MAE (D) | Range (D) | ||
| SRK II | 1.13 | 1.22 | 0.02–4.28 | <0.001 |
| SRK/T | 0.39 | 0.49 | 0.02–2.24 | 0.077 |
| Holladay 1 | 0.46 | 0.61 | 0.02–1.99 | <0.001 |
| Hoffer Q | 0.53 | 0.71 | 0.00–2.45 | <0.001 |
| Haigis | 0.39 | 0.41 | 0.00–1.30 | - |
Table 3.MedAE and MAE as predicted by the SRK/T and Haigis formulas according to the ACD/AL and AL
| Formula | Low ACD/AL (n=30) | High ACD/AL (n=30) | P-valuea) | Low AL (n=33) | High AL (n=27) | P-valueb) | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| MedAE (D) | MAE (D) | MedAE (D) | MAE (D) | MedAE (D) | MAE (D) | MedAE (D) | MAE (D) | |||
| SRK/T | 0.59 | 0.70 | 0.22 | 0.28 | <0.001 | 0.35 | 0.38 | 0.49 | 0.63 | 0.039 |
| Haigis | 0.43 | 0.50 | 0.23 | 0.32 | 0.010 | 0.38 | 0.38 | 0.39 | 0.45 | 0.250 |
| P-valuec) | 0.002 | 0.449 | 0.948 | 0.012 | ||||||
MedAE, median absolute error; MAE, mean absolute error; SRK/T, Sanders-Retzlaff-Kraff theoretical; ACD/AL, anterior chamber depth to axial length ratio; D, diopters.
a)Mann-Whitney test; comparison between low ACD/AL group and high ACD/AL group;
b)Mann-Whitney test; comparison between low AL group and high AL group;
c)Wilcoxon signed rank test; comparison between the SRK/T formula and the Haigis formula.
- 1. Mamalis N. Intraocular lens power accuracy: how are we doing? J Cataract Refract Surg 2003;29:1‒3. ArticlePubMed
- 2. Olsen T. Improved accuracy of intraocular lens power calculation with the Zeiss IOLMaster. Acta Ophthalmol Scand 2007;85:84‒7. ArticlePubMed
- 3. Olsen T. Calculation of intraocular lens power: a review. Acta Ophthalmol Scand 2007;85:472‒85. ArticlePubMed
- 4. Olsen T. Sources of error in intraocular lens power calculation. J Cataract Refract Surg 1992;18:125‒9. ArticlePubMed
- 5. Olsen T, Thorwest M. Calibration of axial length measurements with the Zeiss IOLMaster. J Cataract Refract Surg 2005;31:1345‒50. ArticlePubMed
- 6. Findl O, Kriechbaum K, Sacu S, et al. Influence of operator experience on the performance of ultrasound biometry compared to optical biometry before cataract surgery. J Cataract Refract Surg 2003;29:1950‒5. ArticlePubMed
- 7. Kielhorn I, Rajan MS, Tesha PM, et al. Clinical assessment of the Zeiss IOLMaster. J Cataract Refract Surg 2003;29:518‒22. ArticlePubMed
- 8. Connors R, Boseman P, Olson RJ. Accuracy and reproducibility of biometry using partial coherence interferometry. J Cataract Refract Surg 2002;28:235‒8. ArticlePubMed
- 9. Tsang CS, Chong GS, Yiu EP, Ho CK. Intraocular lens power calculation formulas in Chinese eyes with high axial myopia. J Cataract Refract Surg 2003;29:1358‒64. ArticlePubMed
- 10. Wang JK, Hu CY, Chang SW. Intraocular lens power calculation using the IOLMaster and various formulas in eyes with long axial length. J Cataract Refract Surg 2008;34:262‒7. ArticlePubMed
- 11. Zaldivar R, Shultz MC, Davidorf JM, Holladay JT. Intraocular lens power calculations in patients with extreme myopia. J Cataract Refract Surg 2000;26:668‒74. ArticlePubMed
- 12. MacLaren RE, Sagoo MS, Restori M, Allan BD. Biometry accuracy using zero- and negative-powered intraocular lenses. J Cataract Refract Surg 2005;31:280‒90. ArticlePubMed
- 13. Drews RC. Results in patients with high and low power intraocular lenses. J Cataract Refract Surg 1986;12:154‒7. ArticlePubMed
- 14. Huber C. Effectiveness of intraocular lens calculation in high ametropia. J Cataract Refract Surg 1989;15:667‒72. ArticlePubMed
- 15. Kohnen S, Brauweiler P. First results of cataract surgery and implantation of negative power intraocular lenses in highly myopic eyes. J Cataract Refract Surg 1996;22:416‒20. ArticlePubMed
- 16. Bang S, Edell E, Yu Q, et al. Accuracy of intraocular lens calculations using the IOLMaster in eyes with long axial length and a comparison of various formulas. Ophthalmology 2011;118:503‒6. ArticlePubMed
- 17. Retzlaff JA, Sanders DR, Kraff MC. Development of the SRK/T intraocular lens implant power calculation formula. J Cataract Refract Surg 1990;16:333‒40. ArticlePubMed
- 18. User Group for Laser Interference Biometry (ULIB). Optimized IOL constants for the Zeiss IOLMaster calculated from patient data on file [Internet]. ULIB; c2016 [cited 2026 Jan 12]. Available from: http://ocusoft.de/ulib/c1.htm
- 19. Sheard RM, Smith GT, Cooke DL. Improving the prediction accuracy of the SRK/T formula: the T2 formula. J Cataract Refract Surg 2010;36:1829‒34. ArticlePubMed
- 20. Haigis W. Occurrence of erroneous anterior chamber depth in the SRK/T formula. J Cataract Refract Surg 1993;19:442‒6. ArticlePubMed
- 21. Haigis W. The Haigis formula. In: Shammas HJ, editor. Intraocular lens power calculations. Slack Inc.; 2004. p. 41‒57.
- 22. Kora Y, Koike M, Suzuki Y, et al. Errors in IOL power calculations for axial high myopia. Ophthalmic Surg 1991;22:78‒81. ArticlePubMed
- 23. Haigis W. Intraocular lens calculation in extreme myopia. J Cataract Refract Surg 2009;35:906‒11. ArticlePubMed
- 24. Petermeier K, Gekeler F, Messias A, et al. Intraocular lens power calculation and optimized constants for highly myopic eyes. J Cataract Refract Surg 2009;35:1575‒81. ArticlePubMed
- 25. Rajan MS, Keilhorn I, Bell JA. Partial coherence laser interferometry vs conventional ultrasound biometry in intraocular lens power calculations. Eye (Lond) 2002;16:552‒6. ArticlePubMedPDF
- 26. Eom Y, Kang SY, Song JS, et al. Comparison of Hoffer Q and Haigis formulae for intraocular lens power calculation according to the anterior chamber depth in short eyes. Am J Ophthalmol 2014;157:818‒24. ArticlePubMed
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteImpact of anterior chamber depth to axial length ratio on conventional intraocular lens power calculation formulas performance in axial myopia
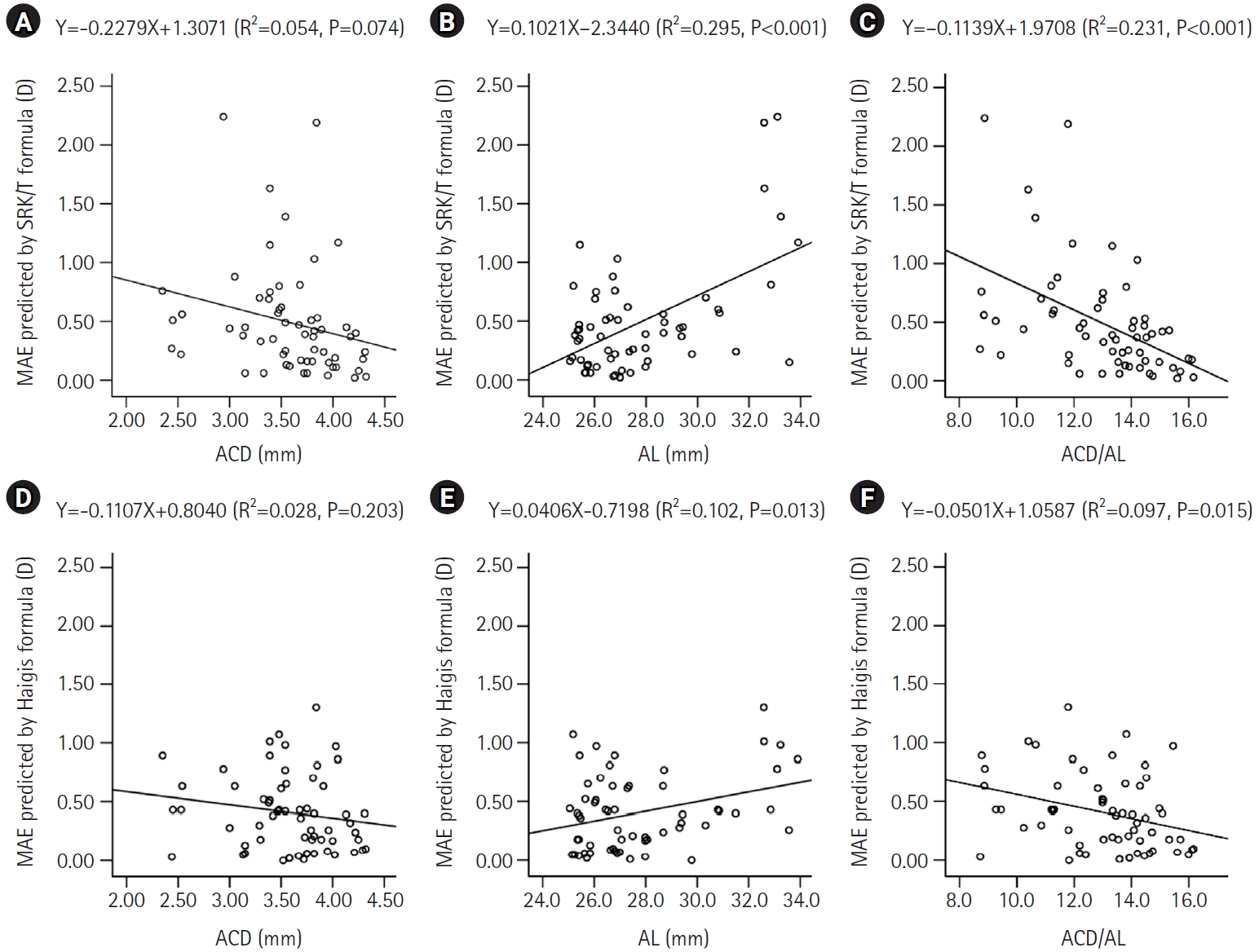
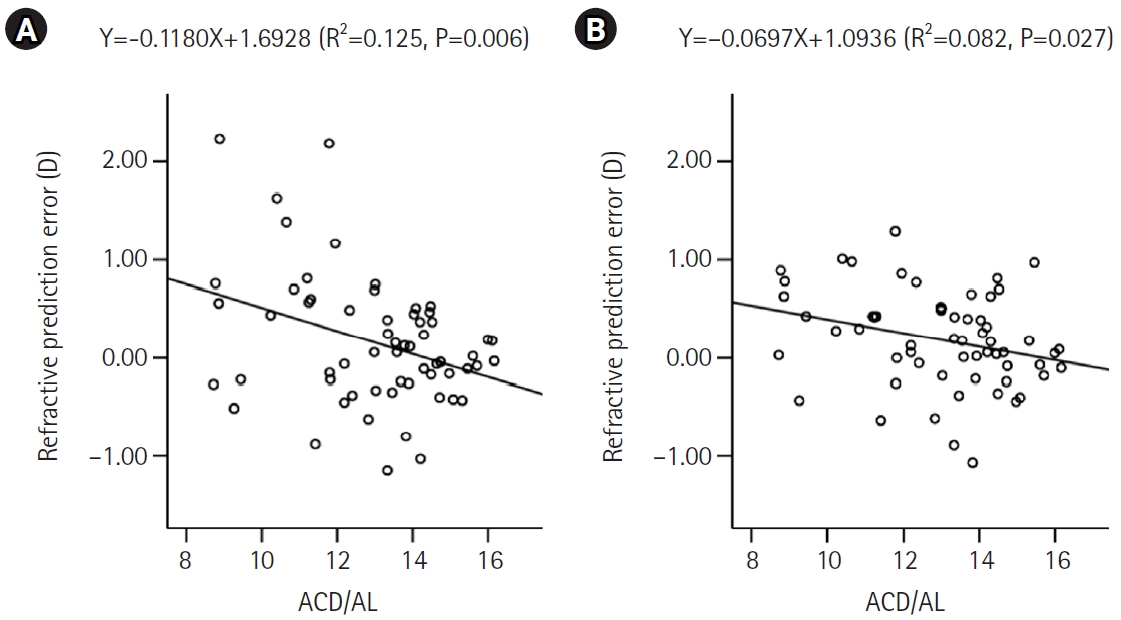
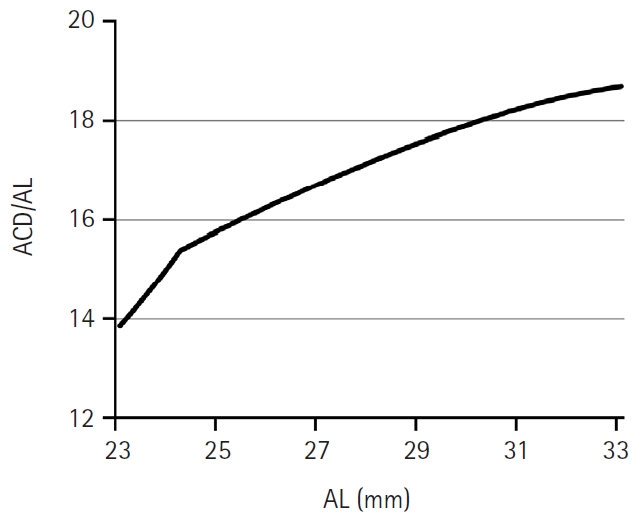
Fig. 1. Linear regression analysis illustrating the relationships among anterior chamber depth (ACD), axial length (AL), the ACD to AL ratio (ACD/AL), and the absolute value of the predicted refractive error calculated using the Sanders-Retzlaff-Kraff theoretical (SRK/T) and Haigis formulas. Panels A–C present the associations for the SRK/T formula with ACD (A), AL (B), and ACD/AL (C), whereas panels D–F depict the corresponding associations for the Haigis formula with ACD (D), AL (E), and ACD/AL (F). MAE, mean absolute error; D, diopters.
Fig. 2. Comparison of the predicted refractive error according to the anterior chamber depth to axial length ratio (ACD/AL) using the Sanders-Retzlaff-Kraff theoretical formula (A) and the Haigis formula (B). D, diopters.
Fig. 3. Graph depicting the theoretical ratio of ACD/AL across varying AL, generated after setting the corneal power to 44.4 diopters, corresponding to the mean corneal power in this study, using the Sanders-Retzlaff-Kraff theoretical formula. ACD/AL, anterior chamber depth to axial length ratio.
Fig. 1.
Fig. 2.
Fig. 3.
Impact of anterior chamber depth to axial length ratio on conventional intraocular lens power calculation formulas performance in axial myopia
| Demographic | Value |
|---|---|
| Age (yr) | 59.6±13.5 (16–83) |
| Sex |
|
| Male | 16 (36.4) |
| Female | 28 (63.6) |
| Laterality |
|
| Right eye | 34 (56.7) |
| Left eye | 26 (43.3) |
| Corneal power (D) | 44.43±1.50 (41.57 to 48.49) |
| Anterior chamber depth (mm) | 3.58±0.48 (2.35 to 4.32) |
| Axial length (mm) | 27.76±2.51 (25.05 to 33.90) |
| IOL power (D) | 9.2±6.7 (–7.0 to 18.0) |
| Formula | Whole subjects (n=60) | P-value |
||
|---|---|---|---|---|
| MedAE (D) | MAE (D) | Range (D) | ||
| SRK II | 1.13 | 1.22 | 0.02–4.28 | <0.001 |
| SRK/T | 0.39 | 0.49 | 0.02–2.24 | 0.077 |
| Holladay 1 | 0.46 | 0.61 | 0.02–1.99 | <0.001 |
| Hoffer Q | 0.53 | 0.71 | 0.00–2.45 | <0.001 |
| Haigis | 0.39 | 0.41 | 0.00–1.30 | - |
| Formula | Low ACD/AL (n=30) | High ACD/AL (n=30) | P-value |
Low AL (n=33) | High AL (n=27) | P-value |
||||
|---|---|---|---|---|---|---|---|---|---|---|
| MedAE (D) | MAE (D) | MedAE (D) | MAE (D) | MedAE (D) | MAE (D) | MedAE (D) | MAE (D) | |||
| SRK/T | 0.59 | 0.70 | 0.22 | 0.28 | <0.001 | 0.35 | 0.38 | 0.49 | 0.63 | 0.039 |
| Haigis | 0.43 | 0.50 | 0.23 | 0.32 | 0.010 | 0.38 | 0.38 | 0.39 | 0.45 | 0.250 |
| P-value |
0.002 | 0.449 | 0.948 | 0.012 | ||||||
Table 1. The clinical and demographic characteristics of the subjects included in the present study (n=60)
Values are presented as mean±standard deviation (range) or number (%). D, diopters. Frequency count.
Table 2. MedAE and MAE as predicted by different formulas
MedAE, median absolute error; MAE, mean absolute error; D, diopters; SRK II, Sanders-Retzlaff-Kraff II; SRK/T, Sanders-Retzlaff-Kraff theoretical. Repeated measures ANOVA (vs. Haigis).
Table 3. MedAE and MAE as predicted by the SRK/T and Haigis formulas according to the ACD/AL and AL
MedAE, median absolute error; MAE, mean absolute error; SRK/T, Sanders-Retzlaff-Kraff theoretical; ACD/AL, anterior chamber depth to axial length ratio; D, diopters. Mann-Whitney test; comparison between low ACD/AL group and high ACD/AL group; Mann-Whitney test; comparison between low AL group and high AL group; Wilcoxon signed rank test; comparison between the SRK/T formula and the Haigis formula.

