
Search
- Page Path
- HOME > Search
Original Articles
- Results of multifocal intraocular lens implantation in patients who underwent corneal refractive surgery
- Eun Chul Kim
- Insights Cataract Refract Surg 2025;10(3):76-82. Published online October 31, 2025
- DOI: https://doi.org/10.63375/icrs.25.011
-
 Abstract
Abstract
 PDF
PDF ePub
ePub - Purpose
The aim of this study was to evaluate the clinical results of multifocal intraocular lenses in patients who underwent corneal refractive surgery.
Methods
Thirty eyes (16 patients; Synergy: ZFR00V) were retrospectively enrolled. Uncorrected and corrected near visual acuity (UNVA, CNVA), intermediate visual acuity (UIVA, CIVA), and distant visual acuity (UDVA, CDVA), manifest refraction spherical equivalent (MRSE), and satisfaction score were assessed before and after surgery.
Results
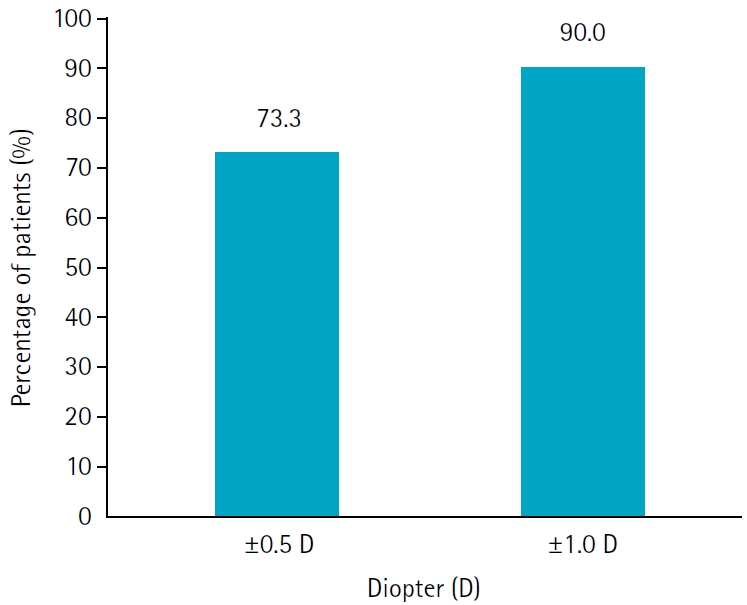
The postoperative UDVA, UIVA, UNVA, and MRSE of the three groups exhibited improvements compared to the preoperative data (P<0.05). The error between the postoperative refraction and the intraocular lens calculation was smaller with the Barrett True K formula than with the Haigis-L formula (P<0.05). The defocus curve at 0 diopter (D) increased, from –1 to –1.5 D, and from –2.5 to –4.0 D, indicating improved vision at distant, intermediate, and near distances. Distance satisfaction (1.47±0.63), near satisfaction (1.25±0.71), and overall satisfaction (1.36±0.42) were good, but light scattering and halo satisfaction (1.97±0.85) yielded a poor result.
Conclusion
In patients with cataracts who underwent corneal refractive surgery, multifocal intraocular lens implantation resulted in excellent uncorrected visual acuity at distant, intermediate, and near distances. However, careful consideration should be given to patient selection due to the incidence of side effects such as glare and halos.
- 910 View
- 14 Download

- Efficacy of extended depth of focus, enhanced monofocal, and monofocal intraocular lenses in patients with retinal disease
- Eun Chul Kim
- Insights Cataract Refract Surg 2025;10(2):52-60. Published online June 30, 2025
- DOI: https://doi.org/10.63375/icrs.25.009
-
Abstract
PDFePub
- Purpose
The aim of this study was to compare the visual quality of extended depth of focus (EDOF), enhanced monofocal, and monofocal intraocular lenses (IOLs) in patients with retinal disease.
Methods
In total, 103 eyes from 93 patients (group 1: enhanced monofocal ICB00, n=36; group 2: EDOF ZXR00, n=36; group 3: monofocal ZCB00, n=31) were retrospectively enrolled. Uncorrected and corrected near visual acuity (UNVA, CNVA), intermediate visual acuity (UIVA, CIVA), and distance visual acuity (UDVA, CDVA), manifest refraction spherical equivalent (MRSE), and satisfaction scores were assessed before and after surgery.
Results
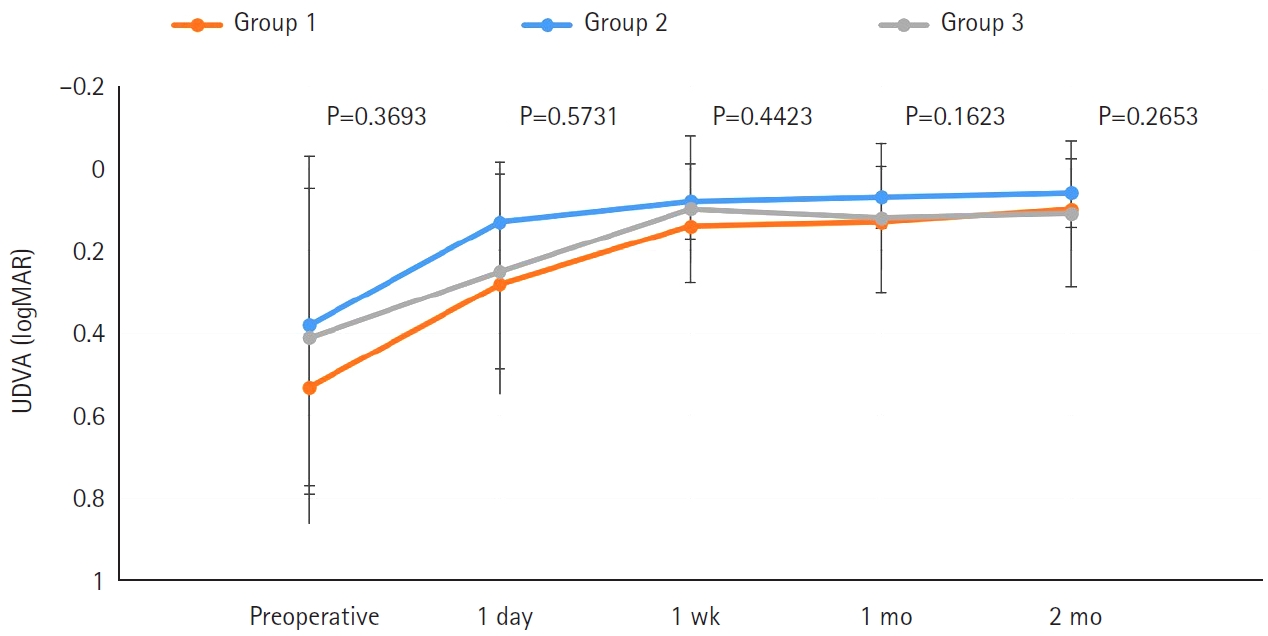
The postoperative UDVA, CDVA, and MRSE of the three groups were better than the preoperative data, respectively (P<0.05). The UIVA of group 1 (0.13±0.12 logMAR) and 2 (0.10±0.11) was significantly better than that of groups 3 (0.25±0.15) (P<0.05). The UNVA of group 2 (0.18±0.12) was significantly better than that of groups 1 (0.32±0.20) and 3 (0.45±0.26; P<0.05). The UDVA of patients with macular edema and macular holes was insignificantly lower than that of epiretinal membranes and high myopia. The overall satisfaction of group 1 (1.58±0.81) and 2 (1.46±0.75) was significantly better than that of groups 3 (1.83±0.97; P<0.05).
Conclusion
EDOF and enhanced monofocal IOLs were associated with better intermediate and near vision than monofocal IOLs in patients with retinal disease. However, monofocal IOLs are recommended in patients with macular edema and macular holes, unlike patients with epiretinal membranes and high myopia.
- 1,560 View
- 21 Download
Review Article
- Selection of an optimal intraocular lens according to the stage of epiretinal membrane
- Sang Beom Han
- Insights Cataract Refract Surg 2025;10(1):7-12. Published online February 28, 2025
- DOI: https://doi.org/10.63375/icrs.25.003
-
Abstract
PDFePub
- Epiretinal membrane (ERM), one of the most common retinal diseases, can cause various degrees of visual disturbance, reduced contrast sensitivity, and metamorphopsia. ERM is not infrequently encountered during preoperative evaluations for cataract surgery, and selecting an appropriate intraocular lens (IOL) according to the location and stage of ERM is necessary in order to improve visual outcomes and patients’ satisfaction. This review summarizes the application of various IOLs—such as multifocal, extended depth of focus, and enhanced monofocal IOLs—in eyes with ERM, and discusses the selection of an appropriate IOL.
-
Citations
Citations to this article as recorded by
- Presbyopia-correcting intraocular lens options in myopic eyes undergoing cataract surgery
Sang Beom Han
Insights in Cataract and Refractive Surgery.2026; 11(1): 1. CrossRef
- Presbyopia-correcting intraocular lens options in myopic eyes undergoing cataract surgery
- 1,806 View
- 19 Download
- 1 Crossref
 First
First Prev
Prev

