
Articles
- Page Path
- HOME > Insights Cataract Refract Surg > Volume 11(2); 2026 > Article
-
Original Article
두 기계에서 회선-직선 복합 방식 초음파유화술과 회선 방식 초음파유화술 비교 -
이지영1, 김은철2

-
Comparison of combined torsional and conventional ultrasound mode versus torsional ultrasound mode phacoemulsification in different machines -
Jiyoung Emily Lee1, Eun Chul Kim2
-
Insights in Cataract and Refractive Surgery 2026;11(2):40-46.
DOI: https://doi.org/10.63375/icrs.25.018
Published online: May 21, 2026
1가톨릭대학교 의과대학 여의도성모병원 안과학교실
2가톨릭대학교 의과대학 부천성모병원 안과학교실
1Department of Ophthalmology, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Department of Ophthalmology, Bucheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- Correspondence to: Eun Chul Kim Department of Ophthalmology, Bucheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 327 Sosa-ro, Wonmi-gu, Bucheon 14647, Korea Tel: +82-32-340-2125 E-mail: eunchol@hanmail.net
• Received: December 28, 2025 • Revised: April 7, 2026 • Accepted: April 7, 2026
© 2026 Korean Society of Cataract and Refractive Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 429 Views
- 4 Download
국문초록
-
목적
- 백내장 수술 시 회선-직선 복합 방식 초음파유화술과 회선 방식 초음파유화술을 사용하였을 때의 임상 결과를 비교하였다.
-
방법
- 백내장 수술을 받은 환자들 중 Cube alpha (Nidek Co.)로 회선-직선 복합 방식 초음파유화술을 사용하여 수술을 시행한 65명의 환자군과 Centurion (Alcon Research Ltd.)으로 회선 운동 방식만을 사용하여 초음파유화술을 시행한 300명의 환자군을 대상으로 수술 후 임상 경과를 비교하였다. Lens Opacities Classification System III에 따라 두 군을 N3, N4, N5, N6로 분류하였으며, 각 군에서 회선-직선군과 회선군의 수술 중 초음파 사용 시간, 누적 소비 에너지, 평형염액 사용량 결과, 수술 후 최대교정시력에 대하여 분석하였다.
-
결과
- N4–6에서 회선군이 회선-직선군에 비하여 초음파 사용 시간과 누적 소비 에너지가 각각 더 높았다(P<0.05). N3–6에서 회선군(N3, 30.97±11.05; N4, 48.56±20.06; N5, 68.27±23.06; N6, 125.64±45.67)의 평형염액 사용량이 회선-직선군(N3, 23.01±10.27; N4, 39.03±24.16; N5, 42.86±18.24; N6, 54.75±0.75)보다 더 많았다(P<0.05). 모든 군에서 수술 후 구면굴절대응치, 각막내피손실, 수술 후 최대교정시력은 통계적으로 유의한 차이가 없었다(P>0.05).
-
결론
- 회선-직선군의 초음파 사용 시간, 누적 소비 에너지, 평형염액 사용량이 회선군에 비하여 효율적이었다. 핵백내장의 경화도가 높은 수술안일수록 회선-직선 복합 방식 초음파유화술이 더 높은 효율을 보이는 것을 확인할 수 있었다.
Abstract
-
Purpose
- This study aimed to compare the clinical outcomes of phacoemulsification performed using a combined torsional and conventional ultrasound mode versus torsional ultrasound mode alone in cataract surgery.
-
Methods
- Sixty-five patients who underwent phacoemulsification using combined torsional and conventional ultrasound mode with the Cube alpha system (Nidek Co.) were compared with 300 patients who underwent phacoemulsification using torsional ultrasound mode alone with the Centurion system (Alcon Research Ltd.). The two groups were classified as N3, N4, N5, or N6 according to the Lens Opacities Classification System III. In each subgroup, phacoemulsification time (seconds), cumulative dissipated energy (CDE), balanced salt solution (BSS) use, and postoperative best-corrected visual acuity were analyzed and compared between the combined-mode group and the torsional-only group.
-
Results
- In the N4–N6 subgroups, the torsional-only group had significantly longer phacoemulsification times and higher CDE values than the combined-mode group (P<0.05 for all comparisons). In the N3–N6 subgroups, the total volume of BSS used in the torsional-only group (N3, 30.97±11.05; N4, 48.56±20.06; N5, 68.27±23.06; N6, 125.64±45.67) was significantly greater than that used in the combined-mode group (N3, 23.01±10.27; N4, 39.03±24.16; N5, 42.86±18.24; N6, 54.75±0.75) (P<0.05). There were no statistically significant differences between the groups in postoperative manifest refraction spherical equivalent, corneal endothelial cell loss, or best-corrected visual acuity.
-
Conclusion
- Compared with torsional ultrasound mode alone, the combined torsional and conventional ultrasound mode was more efficient in terms of ultrasound time, CDE, and BSS use. This advantage was more evident with increasing nuclear sclerosis grade.
서론
방법
결과
고찰
Article Information
Author contributions
Conceptualization: ECK. Data curation: JEL, ECK. Formal analysis: JEL, ECK. Visualization: JEL, ECK. Writing – original draft: JEL, ECK. Writing – review & editing: ECK. Final approval of the manuscript: all authors.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Fig. 1.Intraoperative phacoemulsification time (seconds) of both groups. In N4–6 nucleosclerosis, the torsional group had a longer ultrasound time than the combined group (*P<0.05). a)Phacoemulsification using combined torsional and conventional ultrasound; b)Phacoemulsification using torsional ultrasound alone.
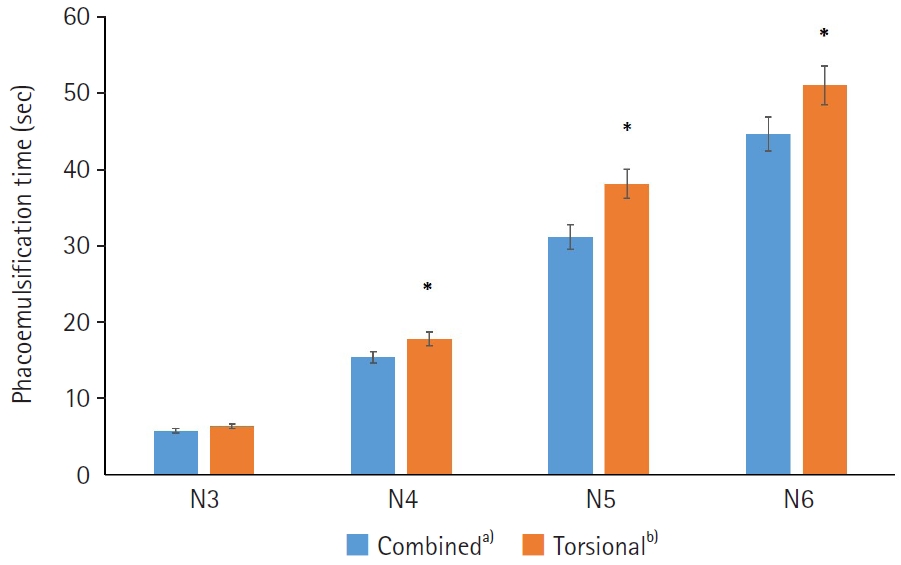
Fig. 2.Intraoperative cumulative dissipated energy of both groups. In N4–6 nucleosclerosis, the torsional group had a higher cumulative dissipated energy than the combined group (*P<0.05). a)Phacoemulsification using combined torsional and conventional ultrasound; b)Phacoemulsification using torsional ultrasound alone.
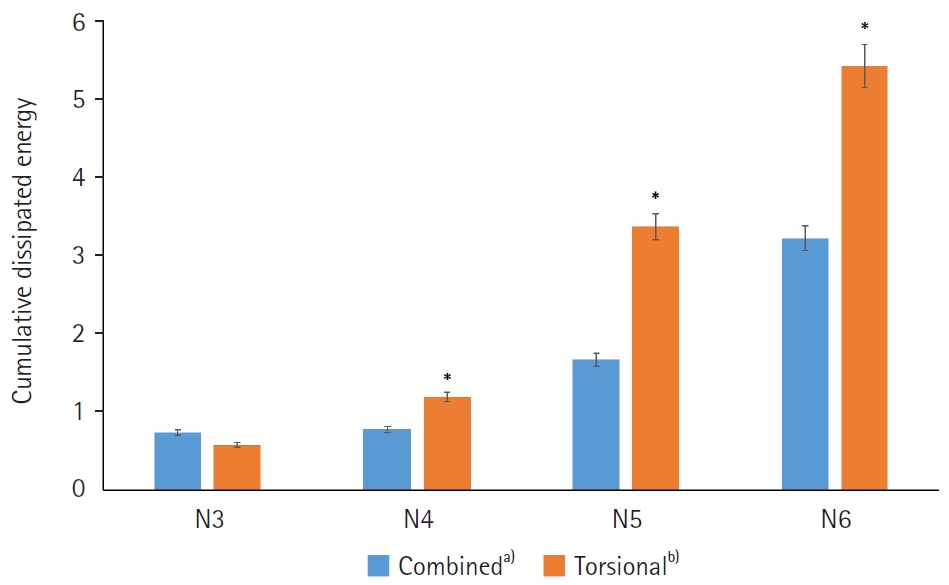
Fig. 3.Intraoperative balanced salt solution (mL) use in both groups. In N3–6 nucleosclerosis, the torsional group had a more balanced salt solution than the combined group (*P<0.05). a)Phacoemulsification using combined torsional and conventional ultrasound; b)Phacoemulsification using torsional ultrasound alone.
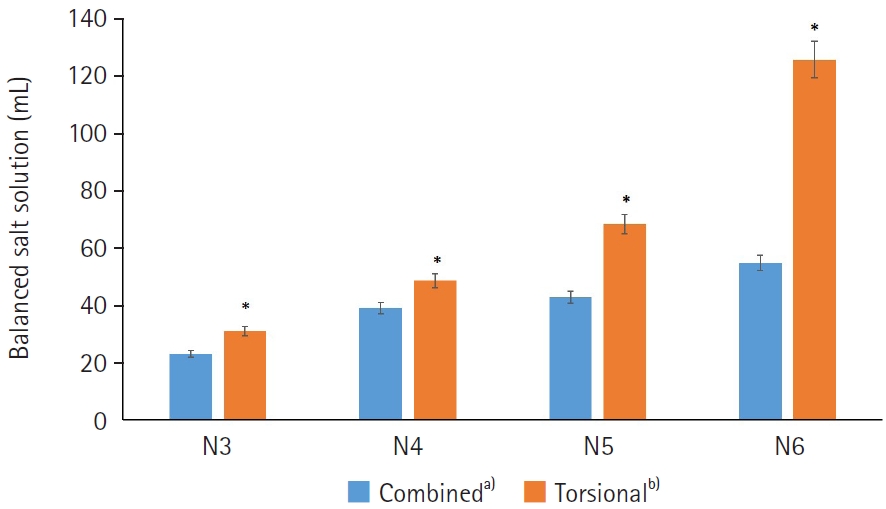
Table 1.Preoperative data of patients
| Parameter | Combineda) | Torsionalb) |
|---|---|---|
| Mean age (yr) | 67.9±9.7 | 67.5±7.2 |
| Sex, male:female | 29:36 | 96:204 |
| MRSE (D) | 1.65±2.17 | 1.73±2.32 |
| BCVA (logMAR) | 0.42±0.26 | 0.44±0.41 |
| Corneal endothelial cell density (cells/mm2) | 2,715.09±395.29 | 2,558.22±432.99 |
| Nucleosclerosis grade | ||
| N3 | 15 | 124 |
| N4 | 29 | 121 |
| N5 | 19 | 41 |
| N6 | 2 | 14 |
| Total no. of eyes | 65 | 300 |
Values are presented as mean±standard deviation. The Mann-Whitney test was used to compare both groups. There was no statistically significant difference in preoperative parameters between the groups.
MRSE, manifest refraction spherical equivalent; D, diopter; BCVA, best-corrected visual acuity; logMAR: logarithm of the minimum angle of resolution.
a)Phacoemulsification using combined torsional and conventional ultrasound;
b)Phacoemulsification using torsional ultrasound alone.
Table 2.Postoperative outcomes at 2 months after surgery
| Parameter | N3 | N4 | N5 | N6 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Combineda) | Torsionalb) | P-value | Combineda) | Torsionalb) | P-value | Combineda) | Torsionalb) | P-value | Combineda) | Torsionalb) | P-value | |
| Age (yr) | 56.67±10.69 | 59.23±9.06 | 0.53 | 70.65±5.54 | 70.64±8.18 | 0.62 | 71.68±8.03 | 73.54±9.62 | 0.45 | 76.50±9.5 | 74.71±9.79 | 0.51 |
| Sex, male:female | 8:7 | 35:89 | - | 9:20 | 43:78 | - | 11:8 | 15:26 | - | 1:1 | 3:11 | - |
| MRSE (D) | –0.42±0.23 | –0.36±0.37 | 0.52 | –0.51±0.28 | –0.48±0.35 | 0.39 | –0.44±0.27 | –0.50±0.36 | 0.38 | –0.43±0.25 | –0.51±0.36 | 0.17 |
| Corneal endothelial cells loss (mm2) | 153.7±53.2 (5.32) | 148.3±48.2 (4.93) | 0.48 | 176.7±58.6 (7.59) | 181.7±60.1 (7.67) | 0.33 | 186.5±62.9 (8.12) | 185.6±59.5 (7.97) | 0.65 | 256.7±95.6 (9.56) | 267.5±89.6 (9.38) | 0.61 |
| Postoperative BCVA (logMAR) | 0.08±0.07 | 0.07±0.09 | 0.59 | 0.10±0.09 | 0.11±0.10 | 0.55 | 0.17±0.11 | 0.18±0.13 | 0.49 | 0.21±0.15 | 0.24±0.18 | 0.37 |
| No. of eyes | 15 | 124 | 29 | 121 | 19 | 41 | 2 | 14 | ||||
Values are presented as mean±standard deviation or mean±standard deviation (%). The Mann-Whitney test was used to compare both groups.
MRSE, manifest refraction spherical equivalent; D, diopter; BCVA, best-corrected visual acuity; logMAR, logarithm of the minimum angle of resolution.
a)Phacoemulsification using combined torsional and conventional ultrasound;
b)Phacoemulsification using torsional ultrasound alone.
- 1. Zacharias J. Role of cavitation in the phacoemulsification process. J Cataract Refract Surg 2008;34:846‒52. ArticlePubMed
- 2. Bozkurt E, Bayraktar S, Yazgan S, et al. Comparison of conventional and torsional mode (OZil) phacoemulsification: randomized prospective clinical study. Eur J Ophthalmol 2009;19:984‒9. ArticlePubMedPDF
- 3. Sippel KC, Pineda R. Phacoemulsification and thermal wound injury. Semin Ophthalmol 2002;17:102‒9. ArticlePubMed
- 4. Kaushik S, Ram J, Brar GS, Bandyopadhyay S. Comparison of the thermal effect on clear corneal incisions during phacoemulsification with different generation machines. Ophthalmic Surg Lasers Imaging 2004;35:364‒70. ArticlePubMed
- 5. Bradley MJ, Olson RJ. A survey about phacoemulsification incision thermal contraction incidence and causal relationships. Am J Ophthalmol 2006;141:222‒4. ArticlePubMed
- 6. Fakhry MA, El Shazly MI. Torsional ultrasound mode versus combined torsional and conventional ultrasound mode phacoemulsification for eyes with hard cataract. Clin Ophthalmol 2011;5:973‒8. ArticlePubMedPMC
- 7. Davison JA. Cumulative tip travel and implied followability of longitudinal and torsional phacoemulsification. J Cataract Refract Surg 2008;34:986‒90. ArticlePubMed
- 8. Liu Y, Zeng M, Liu X, et al. Torsional mode versus conventional ultrasound mode phacoemulsification: randomized comparative clinical study. J Cataract Refract Surg 2007;33:287‒92. ArticlePubMed
- 9. Kim DH, Wee WR, Lee JH, Kim MK. The comparison between torsional and conventional mode phacoemulsification in moderate and hard cataracts. Korean J Ophthalmol 2010;24:336‒40. ArticlePubMedPMC
- 10. Yang WJ, Wang XH, Zhao F, et al. Torsional and burst mode phacoemulsification for patients with hard nuclear cataract: a randomized control study. Medicine (Baltimore) 2019;98:e15870. ArticlePubMedPMC
- 11. Chen X, Ji Y, Lu Y. Comparison of clear corneal incision injuries between torsional and conventional phacoemulsification. Graefes Arch Clin Exp Ophthalmol 2013;251:2147‒54. ArticlePubMedPDF
- 12. Reuschel A, Bogatsch H, Barth T, Wiedemann R. Comparison of endothelial changes and power settings between torsional and longitudinal phacoemulsification. J Cataract Refract Surg 2010;36:1855‒61. ArticlePubMed
- 13. Zeng M, Liu X, Liu Y, et al. Torsional ultrasound modality for hard nucleus phacoemulsification cataract extraction. Br J Ophthalmol 2008;92:1092‒6. ArticlePubMedPMC
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteComparison of combined torsional and conventional ultrasound mode versus torsional ultrasound mode phacoemulsification in different machines
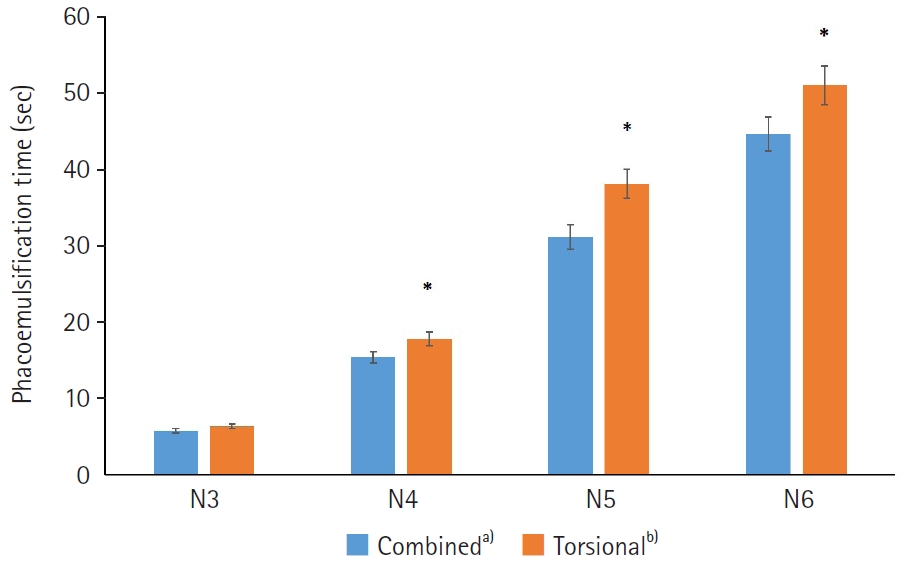
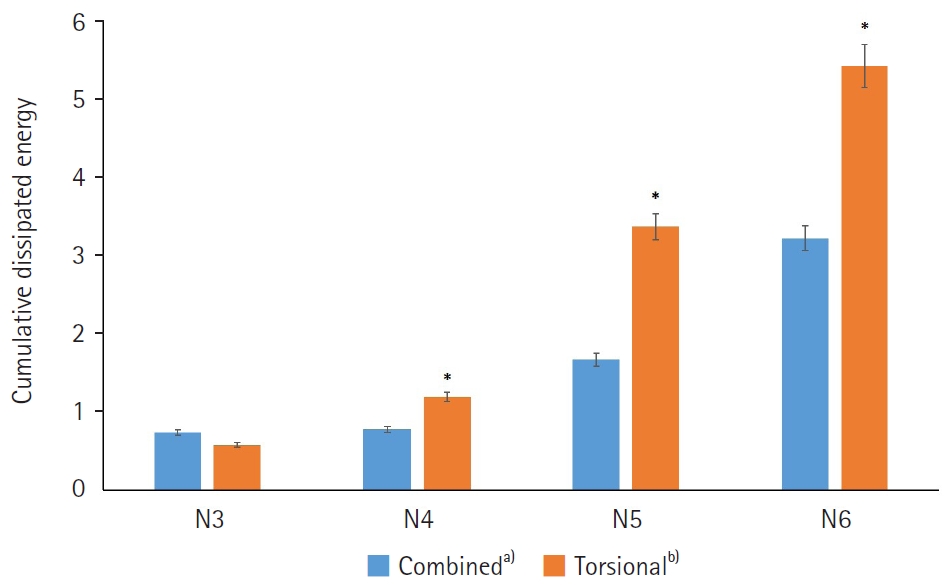
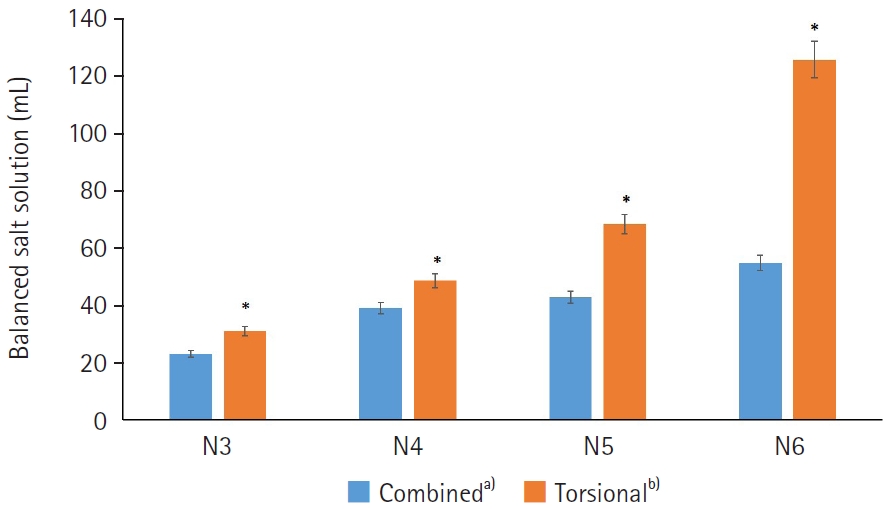
Fig. 1. Intraoperative phacoemulsification time (seconds) of both groups. In N4–6 nucleosclerosis, the torsional group had a longer ultrasound time than the combined group (*P<0.05). a)Phacoemulsification using combined torsional and conventional ultrasound; b)Phacoemulsification using torsional ultrasound alone.
Fig. 2. Intraoperative cumulative dissipated energy of both groups. In N4–6 nucleosclerosis, the torsional group had a higher cumulative dissipated energy than the combined group (*P<0.05). a)Phacoemulsification using combined torsional and conventional ultrasound; b)Phacoemulsification using torsional ultrasound alone.
Fig. 3. Intraoperative balanced salt solution (mL) use in both groups. In N3–6 nucleosclerosis, the torsional group had a more balanced salt solution than the combined group (*P<0.05). a)Phacoemulsification using combined torsional and conventional ultrasound; b)Phacoemulsification using torsional ultrasound alone.
Fig. 1.
Fig. 2.
Fig. 3.
Comparison of combined torsional and conventional ultrasound mode versus torsional ultrasound mode phacoemulsification in different machines
| Parameter | Combined |
Torsional |
|---|---|---|
| Mean age (yr) | 67.9±9.7 | 67.5±7.2 |
| Sex, male:female | 29:36 | 96:204 |
| MRSE (D) | 1.65±2.17 | 1.73±2.32 |
| BCVA (logMAR) | 0.42±0.26 | 0.44±0.41 |
| Corneal endothelial cell density (cells/mm2) | 2,715.09±395.29 | 2,558.22±432.99 |
| Nucleosclerosis grade | ||
| N3 | 15 | 124 |
| N4 | 29 | 121 |
| N5 | 19 | 41 |
| N6 | 2 | 14 |
| Total no. of eyes | 65 | 300 |
| Parameter | N3 | N4 | N5 | N6 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Combined |
Torsional |
P-value | Combined |
Torsional |
P-value | Combined |
Torsional |
P-value | Combined |
Torsional |
P-value | |
| Age (yr) | 56.67±10.69 | 59.23±9.06 | 0.53 | 70.65±5.54 | 70.64±8.18 | 0.62 | 71.68±8.03 | 73.54±9.62 | 0.45 | 76.50±9.5 | 74.71±9.79 | 0.51 |
| Sex, male:female | 8:7 | 35:89 | - | 9:20 | 43:78 | - | 11:8 | 15:26 | - | 1:1 | 3:11 | - |
| MRSE (D) | –0.42±0.23 | –0.36±0.37 | 0.52 | –0.51±0.28 | –0.48±0.35 | 0.39 | –0.44±0.27 | –0.50±0.36 | 0.38 | –0.43±0.25 | –0.51±0.36 | 0.17 |
| Corneal endothelial cells loss (mm2) | 153.7±53.2 (5.32) | 148.3±48.2 (4.93) | 0.48 | 176.7±58.6 (7.59) | 181.7±60.1 (7.67) | 0.33 | 186.5±62.9 (8.12) | 185.6±59.5 (7.97) | 0.65 | 256.7±95.6 (9.56) | 267.5±89.6 (9.38) | 0.61 |
| Postoperative BCVA (logMAR) | 0.08±0.07 | 0.07±0.09 | 0.59 | 0.10±0.09 | 0.11±0.10 | 0.55 | 0.17±0.11 | 0.18±0.13 | 0.49 | 0.21±0.15 | 0.24±0.18 | 0.37 |
| No. of eyes | 15 | 124 | 29 | 121 | 19 | 41 | 2 | 14 | ||||
Table 1. Preoperative data of patients
Values are presented as mean±standard deviation. The Mann-Whitney test was used to compare both groups. There was no statistically significant difference in preoperative parameters between the groups. MRSE, manifest refraction spherical equivalent; D, diopter; BCVA, best-corrected visual acuity; logMAR: logarithm of the minimum angle of resolution. Phacoemulsification using combined torsional and conventional ultrasound; Phacoemulsification using torsional ultrasound alone.
Table 2. Postoperative outcomes at 2 months after surgery
Values are presented as mean±standard deviation or mean±standard deviation (%). The Mann-Whitney test was used to compare both groups. MRSE, manifest refraction spherical equivalent; D, diopter; BCVA, best-corrected visual acuity; logMAR, logarithm of the minimum angle of resolution. Phacoemulsification using combined torsional and conventional ultrasound; Phacoemulsification using torsional ultrasound alone.

